

Desvenlafaxine Versus Placebo in a Fluoxetine-Referenced Study of Children and Adolescents with Major Depressive Disorder
- PMID: 29189044
- PMCID: PMC5771543
- DOI: 10.1089/cap.2017.0100
Desvenlafaxine Versus Placebo in a Fluoxetine-Referenced Study of Children and Adolescents with Major Depressive Disorder
Abstract
Objectives: To evaluate the short-term efficacy and safety of desvenlafaxine (25-50 mg/d) compared with placebo in children and adolescents with major depressive disorder (MDD).
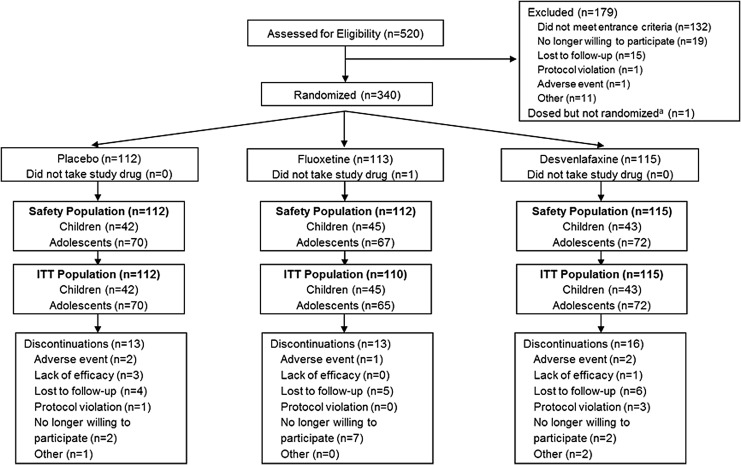
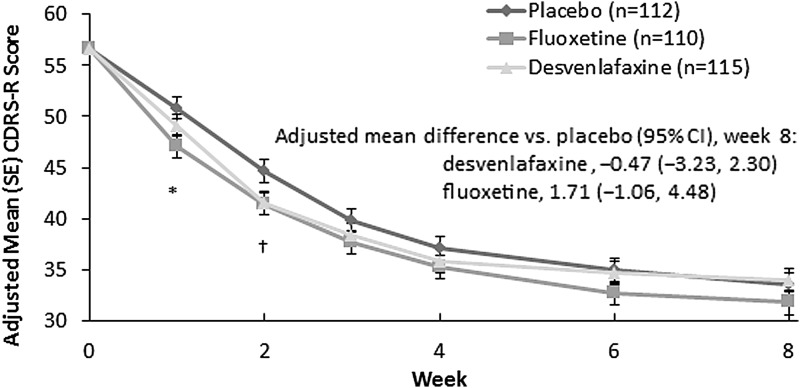
Methods: Outpatient children (7-11 years) and adolescents (12-17 years) who met DSM-IV-TR criteria for MDD and had screening and baseline Children's Depression Rating Scale-Revised (CDRS-R) total scores >40 were randomly assigned to 8-week treatment with placebo, desvenlafaxine (25, 35, or 50 mg/d based on baseline weight), or fluoxetine (20 mg/d). The primary efficacy endpoint was change from baseline in CDRS-R total score at week 8, analyzed using a mixed-effects model for repeated measures. Secondary efficacy endpoints included week 8 Clinical Global Impressions-Severity, Clinical Global Impressions-Improvement (CGI-I), and response (CGI-I ≤ 2). Safety assessments included adverse events, physical and vital sign measurements, laboratory evaluations, electrocardiogram, and the Columbia-Suicide Severity Rating Scale.
Results: The safety population included 339 patients (children, n = 130; adolescents, n = 209). The primary endpoint, change from baseline in CDRS-R total score at week 8, did not statistically separate from placebo, for either desvenlafaxine (adjusted mean [standard error] change, -22.6 [1.17]) or fluoxetine (-24.8 [1.17]; placebo, -23.1 [1.18]). Week 8 CGI-I response rates were significantly greater for fluoxetine (78.2%; p = 0.017) than for placebo (62.6%); desvenlafaxine (68.7%) did not differ from placebo. Other secondary outcomes were consistent with those obtained with CDRS-R. Rates of treatment-emergent adverse events were comparable among treatment groups (desvenlafaxine, 60.0%; placebo, 70.5%; and fluoxetine, 64.3%).
Conclusion: Desvenlafaxine did not demonstrate efficacy for treating MDD in children and adolescents in this trial. Because neither desvenlafaxine nor the reference medication, fluoxetine, demonstrated a statistically significant difference from placebo on the primary endpoint, this was considered a failed trial and no efficacy conclusions can be drawn. Desvenlafaxine 25-50 mg/d was generally safe and well tolerated in children and adolescents in this study.
Keywords: adolescents; children; clinical trial; desvenlafaxine; major depressive disorder; treatment efficacy.
Figures
References
-
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision. Washington, DC: American Psychiatric Association; 2000
-
- Atkinson SD, Prakash A, Zhang Q, Pangallo BA, Bangs ME, Emslie GJ, March JS: A double-blind efficacy and safety study of duloxetine flexible dosing in children and adolescents with major depressive disorder. J Child Adolesc Psychopharmacol 24:180–189, 2014 - PubMed
-
- Birmaher B, Brent D, Bernet W, Bukstein O, Walter H, Benson RS, Chrisman A, Farchione T, Greenhill L, Hamilton J, Keable H, Kinlan J, Schoettle U, Stock S, Ptakowski KK, Medicus J: Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. J Am Acad Child Adolesc Psychiatry 46:1503–1526, 2007 - PubMed
-
- Birmaher B, Ryan ND, Williamson DE, Brent DA, Kaufman J, Dahl RE, Perel J, Nelson B: Childhood and adolescent depression: A review of the past 10 years. Part I. J Am Acad Child Adolesc Psychiatry 35:1427–1439, 1996 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous