

Metachronous colorectal cancer following segmental or extended colectomy in Lynch syndrome: a systematic review and meta-analysis
- PMID: 29189962
- PMCID: PMC6182577
- DOI: 10.1007/s10689-017-0062-2
Metachronous colorectal cancer following segmental or extended colectomy in Lynch syndrome: a systematic review and meta-analysis
Abstract
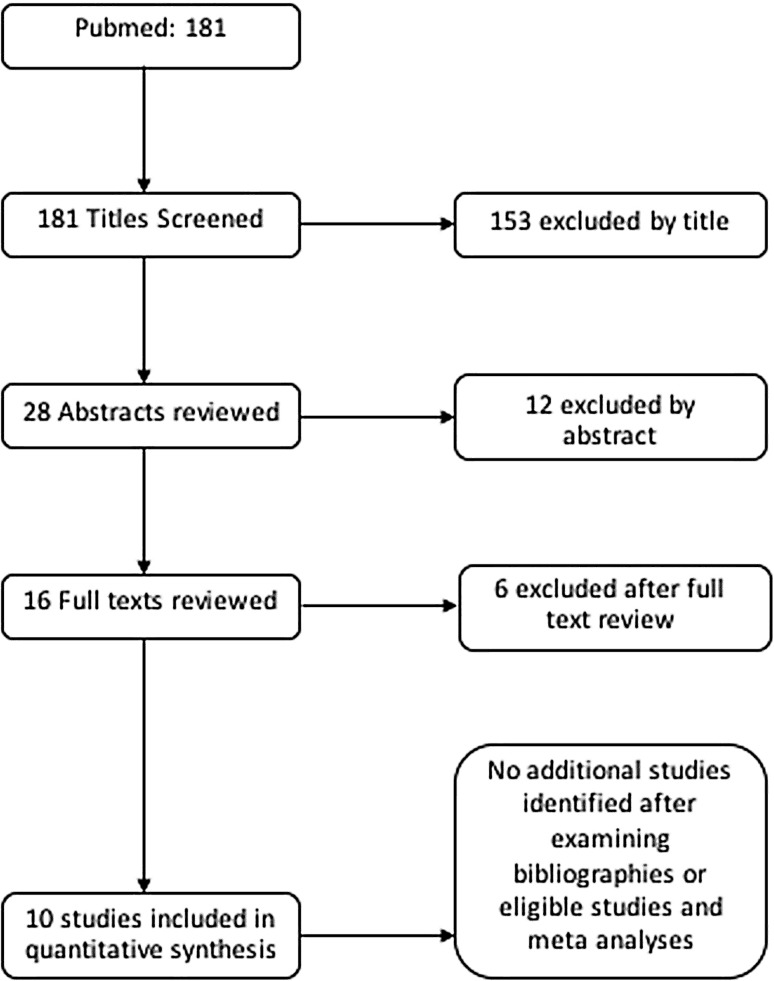
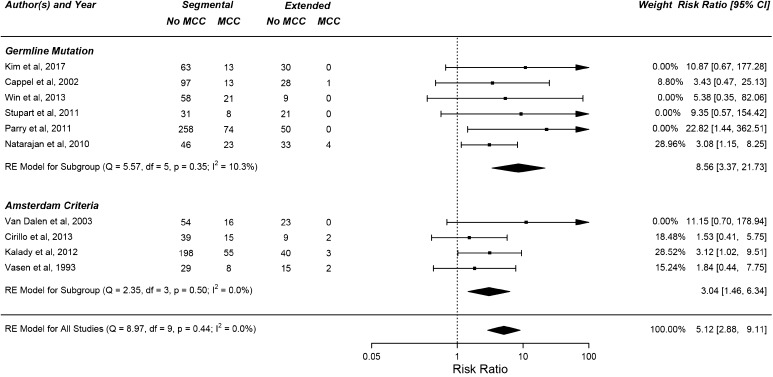
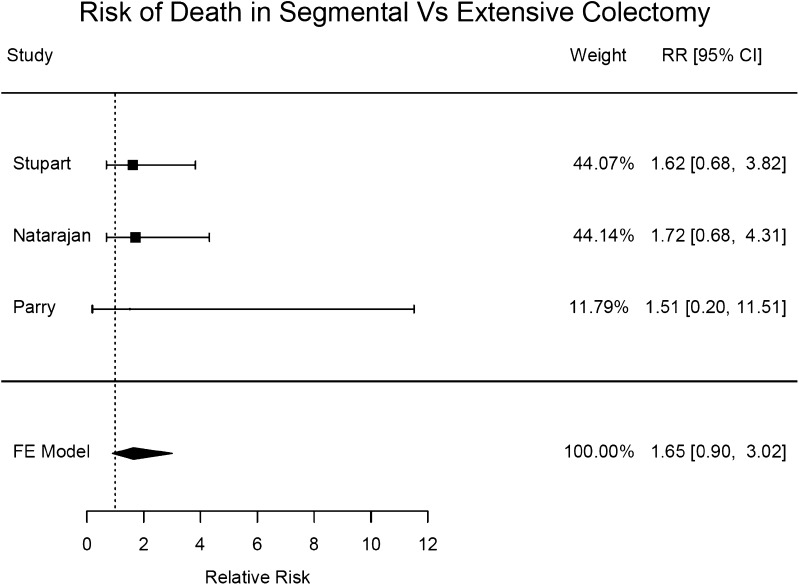
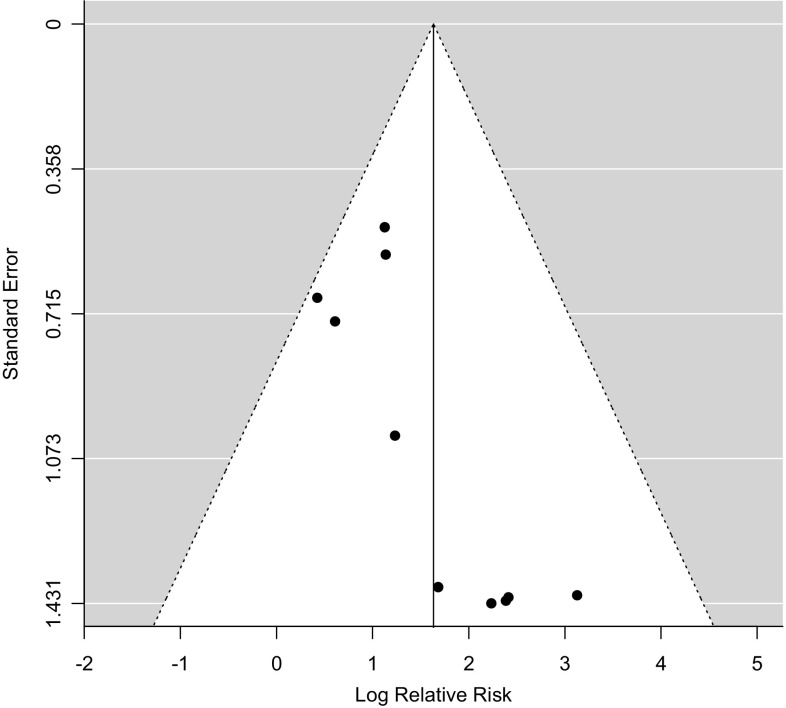
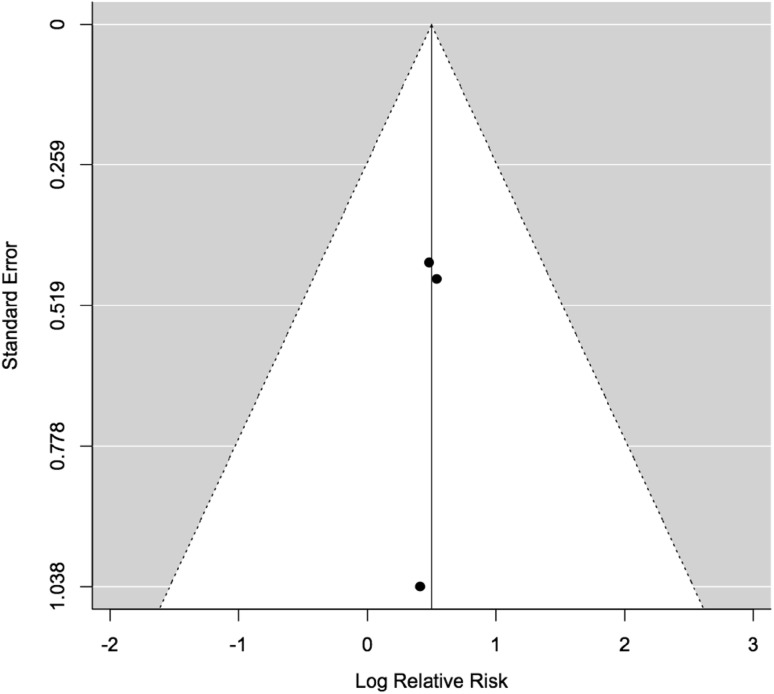
Around 5% of colorectal cancers are due to mutations within DNA mismatch repair genes, resulting in Lynch syndrome (LS). These mutations have a high penetrance with early onset of colorectal cancer at a mean age of 45 years. The mainstay of surgical management is either a segmental or extensive colectomy. Currently there is no unified agreement as to which management strategy is superior due to limited conclusive empirical evidence available. A systematic review and meta- analysis to evaluate the risk of metachronous colorectal cancer (MCC) and mortality in LS following segmental and extensive colectomy. A systematic review of the PubMed database was conducted. Studies were included/ excluded based on pre-specified criteria. To assess the risk of MCC and mortality attributed to segmental or extensive colectomies, relative risks (RR) were calculated and corresponding 95% confidence intervals (CI). Publication bias was investigated using funnel plots. Data about mortality, as well as patient ascertainment [Amsterdam criteria (AC), germline mutation (GM)] were also extracted. Statistical analysis was conducted using the R program (version 3.2.3). The literature search identified 85 studies. After further analysis ten studies were eligible for inclusion in data synthesis. Pooled data identified 1389 patients followed up for a mean of 100.7 months with a mean age of onset of 45.5 years of age. A total 1119 patients underwent segmental colectomies with an absolute risk of MCC in this group of 22.4% at the end of follow-up. The 270 patients who had extensive colectomies had a MCC absolute risk of 4.7% (0% in those with a panproctocolecomy). Segmental colectomy was significantly associated with an increased relative risk of MCC (RR = 5.12; 95% CI 2.88-9.11; Fig. 1), although no significant association with mortality was identified (RR = 1.65; 95% CI 0.90-3.02). There was no statistically significant difference in the risk of MCC between AC and GM cohorts (p = 0.5, Chi-squared test). In LS, segmental colectomy results in a significant increased risk of developing MCC. Despite the choice of segmental or extensive colectomies having no statistically significant impact on mortality, the choice of initial surgical management can impact a patient's requirement for further surgery. An extensive colectomy can result in decreased need for further surgery; reduced hospital stays and associated costs. The significant difference in the risk of MCC, following segmental or extensive colectomies should be discussed with patients when deciding appropriate management. An individualised approach should be utilised, taking into account the patient's age, co-morbidities and genotype. In order to determine likely germline-specific effects, or a difference in survival, larger and more comprehensive studies are required.
Keywords: Amsterdam criteria; Colectomy; Colorectal cancer; Lynch syndrome; Metachronous colorectal cancer.
Figures
Comment in
-
Letter to the editor.Fam Cancer. 2018 Oct;17(4):565-566. doi: 10.1007/s10689-018-0069-3. Fam Cancer. 2018. PMID: 29330737 No abstract available.
-
Response to letter to editor regarding published article-metachronous colorectal cancer following segmental or extended colectomy in Lynch syndrome: a systematic review and meta-analysis.Fam Cancer. 2018 Oct;17(4):545-546. doi: 10.1007/s10689-018-0077-3. Fam Cancer. 2018. PMID: 29450672 No abstract available.
Similar articles
-
Risk of metachronous colorectal cancer following colectomy in Lynch syndrome: a systematic review and meta-analysis.Colorectal Dis. 2017 Jun;19(6):528-536. doi: 10.1111/codi.13679. Colorectal Dis. 2017. PMID: 28407411
-
Survival Outcome and Risk of Metachronous Colorectal Cancer After Surgery in Lynch Syndrome.Ann Surg Oncol. 2017 Apr;24(4):1085-1092. doi: 10.1245/s10434-016-5633-1. Epub 2016 Oct 20. Ann Surg Oncol. 2017. PMID: 27766559
-
Segmental versus extended colectomy for colorectal cancer in patients with lynch syndrome: A systematic review and meta-analysis.World J Surg. 2025 Jan;49(1):24-33. doi: 10.1002/wjs.12443. Epub 2024 Dec 4. World J Surg. 2025. PMID: 39631798
-
Metachronous serrated neoplasia is uncommon after right colectomy in patients with methylator colon cancers with a high degree of microsatellite instability.Dis Colon Rectum. 2014 Jan;57(1):39-46. doi: 10.1097/01.dcr.0000437690.18709.76. Dis Colon Rectum. 2014. PMID: 24316944
-
Risk of Metachronous Colorectal Neoplasm after a Segmental Colectomy in Lynch Syndrome Patients According to Mismatch Repair Gene Status.J Am Coll Surg. 2020 Apr;230(4):669-675. doi: 10.1016/j.jamcollsurg.2020.01.005. Epub 2020 Jan 30. J Am Coll Surg. 2020. PMID: 32007537 Free PMC article.
Cited by
-
Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG).Gut. 2020 Mar;69(3):411-444. doi: 10.1136/gutjnl-2019-319915. Epub 2019 Nov 28. Gut. 2020. PMID: 31780574 Free PMC article.
-
Metachronous colorectal cancer risks after extended or segmental resection in MLH1, MSH2, and MSH6 Lynch syndrome: multicentre study from the Prospective Lynch Syndrome Database.Br J Surg. 2025 Mar 28;112(4):znaf061. doi: 10.1093/bjs/znaf061. Br J Surg. 2025. PMID: 40231433 Free PMC article.
-
Delphi Initiative for Early-Onset Colorectal Cancer (DIRECt) International Management Guidelines.Clin Gastroenterol Hepatol. 2023 Mar;21(3):581-603.e33. doi: 10.1016/j.cgh.2022.12.006. Epub 2022 Dec 20. Clin Gastroenterol Hepatol. 2023. PMID: 36549470 Free PMC article.
-
European guidelines from the EHTG and ESCP for Lynch syndrome: an updated third edition of the Mallorca guidelines based on gene and gender.Br J Surg. 2021 May 27;108(5):484-498. doi: 10.1002/bjs.11902. Br J Surg. 2021. PMID: 34043773 Free PMC article.
-
Current practice of colonoscopy surveillance in patients with lynch syndrome: A multicenter retrospective cohort study in Japan.DEN Open. 2022 Nov 1;3(1):e179. doi: 10.1002/deo2.179. eCollection 2023 Apr. DEN Open. 2022. PMID: 36330234 Free PMC article.
References
-
- World Health Organisation (2017) http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx. Accessed 6 June 2017
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
