

Potential of Noncontrast Magnetic Resonance Imaging With Diffusion-Weighted Imaging in Characterization of Breast Lesions: Intraindividual Comparison With Dynamic Contrast-Enhanced Magnetic Resonance Imaging
- PMID: 29190227
- PMCID: PMC8158059
- DOI: 10.1097/RLI.0000000000000433
Potential of Noncontrast Magnetic Resonance Imaging With Diffusion-Weighted Imaging in Characterization of Breast Lesions: Intraindividual Comparison With Dynamic Contrast-Enhanced Magnetic Resonance Imaging
Abstract
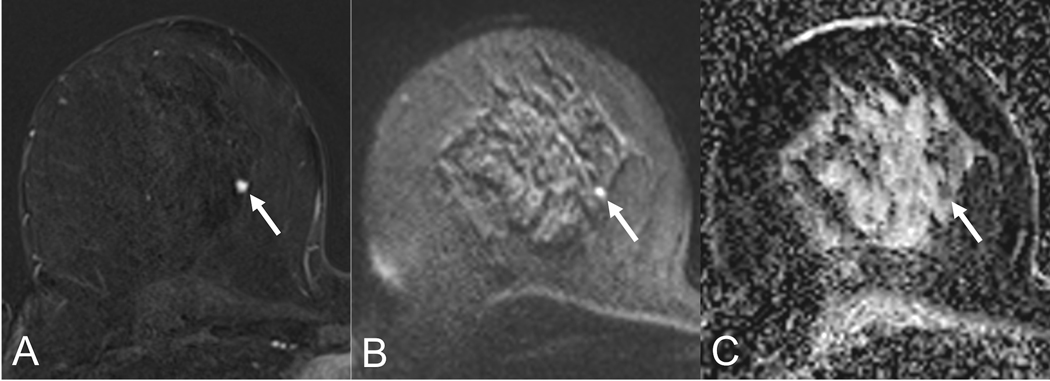
Objectives: The aim of this study was to assess the potential of noncontrast magnetic resonance imaging (NC-MRI) with diffusion-weighted imaging (DWI) in characterization of breast lesions in comparison to dynamic contrast-enhanced MRI (DCE-MRI) at 3 T.
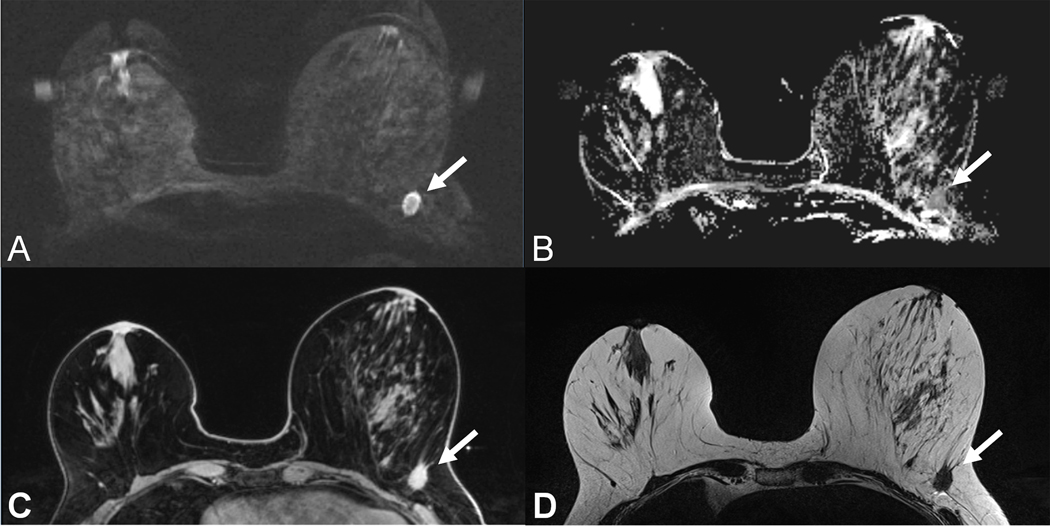
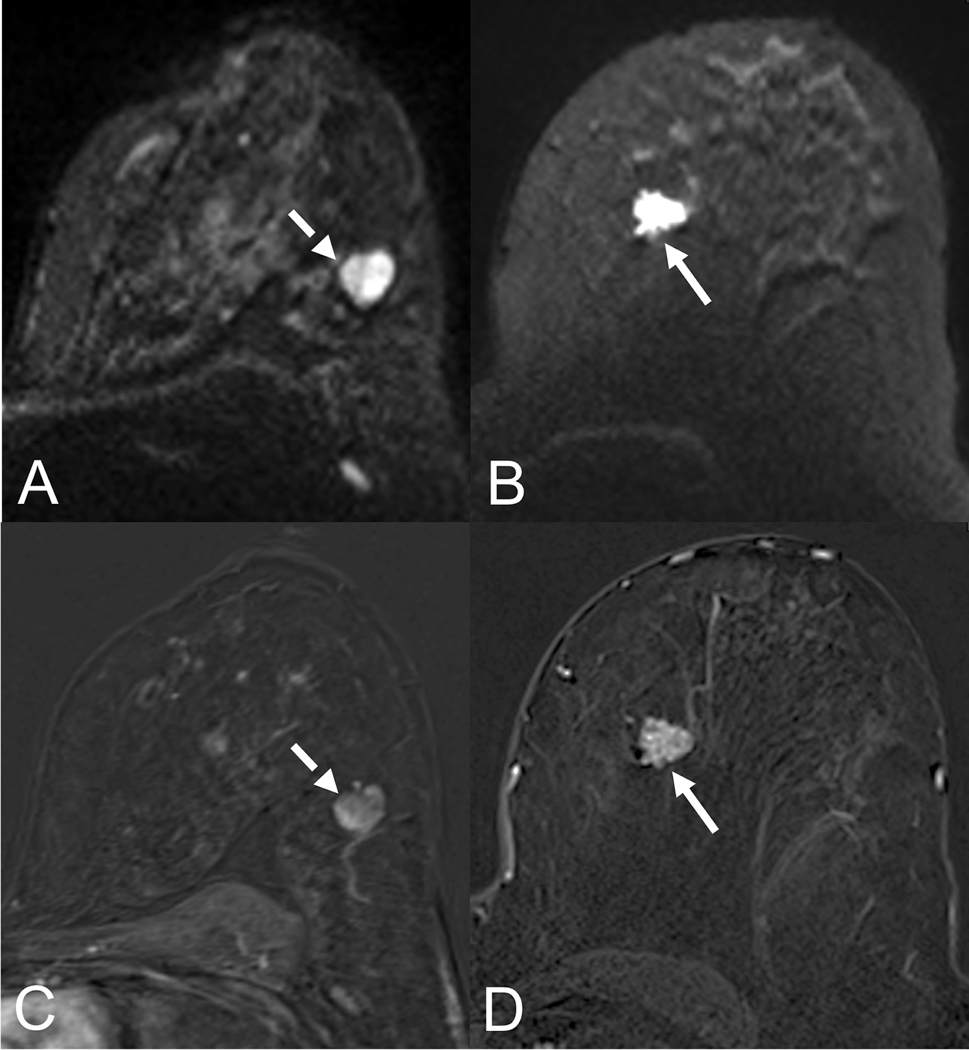
Materials and methods: Consecutive patients with conventional imaging (mammography, ultrasound) BI-RADS 4/5 findings were included in this institutional review board-approved single-center study. All underwent 3 T breast MRI including readout-segmented DWI, DCE, and T2-weighted sequences. Final diagnosis was defined by histopathology or follow-up (>24 months). Two experienced radiologists (R1, R2) independently assigned lesion conspicuity (0 = minimal to 3 = excellent) and BI-RADS scores to NC-MRI (readout-segmented DWI including apparent diffusion coefficient maps) and DCE-MRI (DCE and T2-weighted). Receiver operating characteristics, κ statistics, and visual grading characteristics analysis were applied.
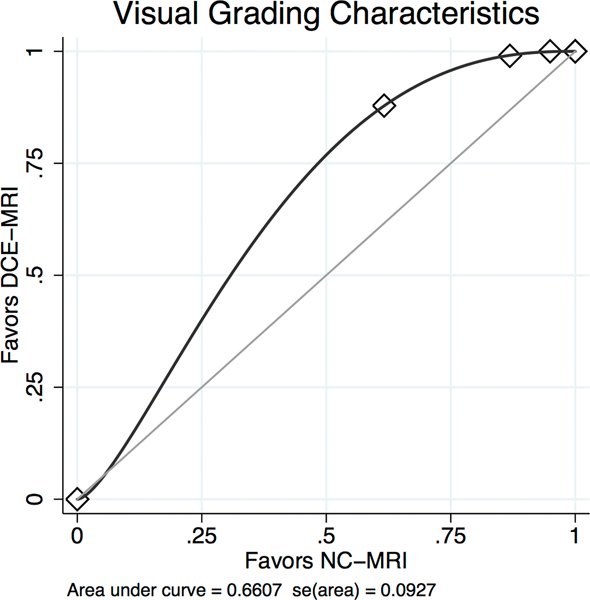
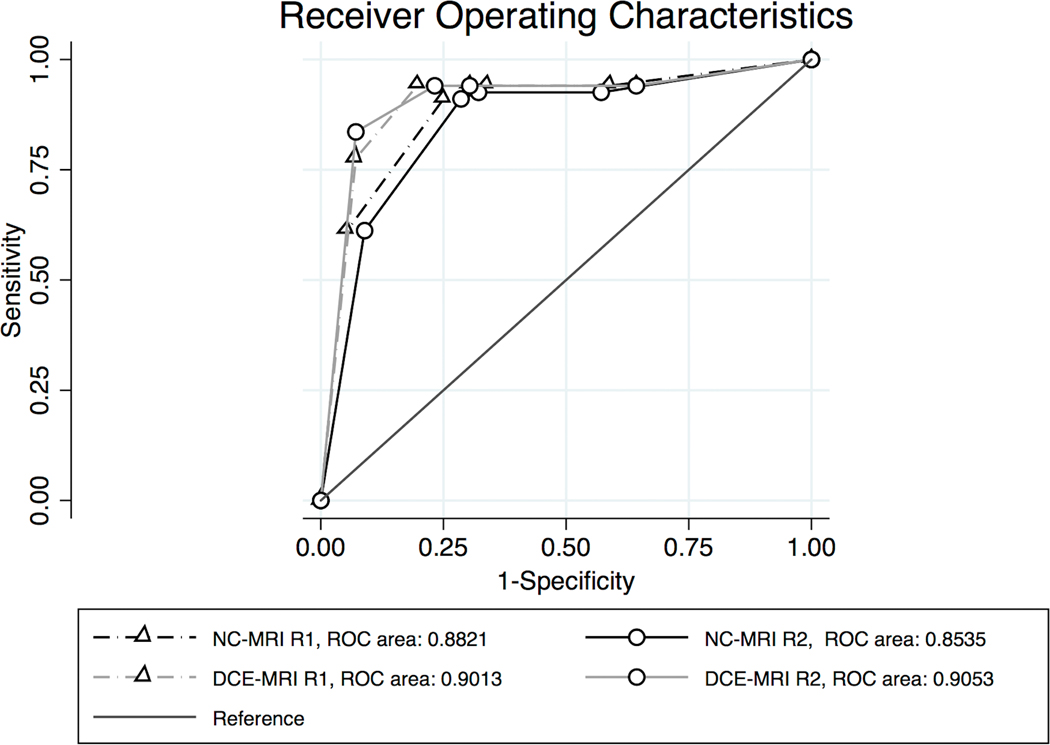
Results: Sixty-seven malignant and 56 benign lesions were identified in 113 patients (mean age, 54 ± 14 years). Areas under the receiver operating characteristics curves were similar: DCE-MRI: 0.901 (R1), 0.905 (R2); NC-MRI: 0.882 (R1), 0.854 (R2); P > 0.05, respectively. The κ agreement was 0.968 (DCE-MRI) and 0.893 (NC-MRI). Visual grading characteristics analysis revealed superior lesion conspicuity by DCE-MRI (0.661, P < 0.001).
Conclusions: Diagnostic performance and interreader agreement of both NC-MRI and DCE-MRI is high, indicating a potential use of NC-MRI as an alternative to DCE-MRI. However, inferior lesion conspicuity and lower interreader agreement of NC-MRI need to be considered.
Figures
References
-
- Warner E, Messersmith H, Causer P, et al. Systematic review: using magnetic resonance imaging to screen women at high risk for breast cancer. Ann. Intern. Med 2008;148(9):671–679. - PubMed
-
- Houssami N, Ciatto S, Macaskill P, et al. Accuracy and surgical impact of magnetic resonance imaging in breast cancer staging: systematic review and meta-analysis in detection of multifocal and multicentric cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol 2008;26(19):3248–3258. - PubMed
-
- Mann RM, Mus RD, van Zelst J, et al. A novel approach to contrast-enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest. Radiol 2014;49(9):579–585. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
