

Association of Quantitative Metastatic Lymph Node Burden With Survival in Hypopharyngeal and Laryngeal Cancer
- PMID: 29192305
- PMCID: PMC6584272
- DOI: 10.1001/jamaoncol.2017.3852
Association of Quantitative Metastatic Lymph Node Burden With Survival in Hypopharyngeal and Laryngeal Cancer
Abstract
Importance: Nodal staging for laryngohypopharyngeal cancers is based primarily on size and laterality, with less value placed on absolute number of metastatic lymph nodes (LNs). We are aware of no studies to date that have specifically addressed the prognostic effect of quantitative nodal burden in larynx or hypopharynx malignancies.
Objective: To assess the independent impact of quantitative metastatic LN burden on mortality risk.
Design, setting, and participants: Univariate and multivariable models were constructed to evaluate the association between patients' number of metastatic LNs and their survival, adjusting for factors such as nodal size, laterality, extranodal extension, margin status, and adjuvant treatment. Participants were patients with squamous cell carcinoma of the larynx or hypopharynx undergoing upfront surgical resection for curative intent at a US hospital between 2004 and 2013, as identified in the National Cancer Database. A neck dissection of a minimum of 10 LNs was required.
Main outcomes and measures: Overall survival.
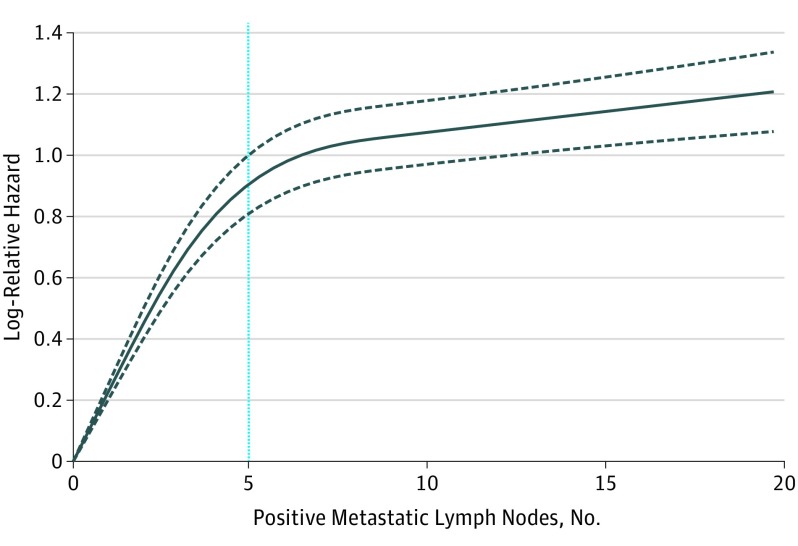
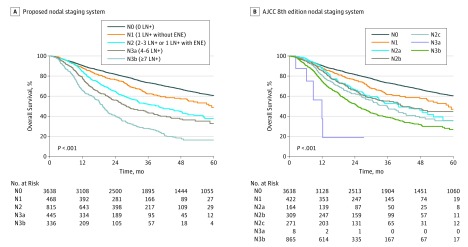
Results: Overall, 8351 cases were included (mean [SD] age, 61 [10.1] years; 6499 men [77.8%]; 4710 patients with metastatic LNs and 3641 with no metastatic LNs). Mortality risk escalated continuously without plateau as number of metastatic nodes increased, with the hazard per node (hazard ratio [HR], 1.19; 95% CI, 1.16-1.23; P < .001) most pronounced up to 5 positive LNs. Extranodal extension was also associated with increased mortality (HR, 1.34; 95% CI, 1.13-1.59; P < .001). Increasing number of nodes examined was associated with improved survival, albeit to a lesser degree (per 10 LNs: HR, 0.97; 95% CI, 0.96-0.98; P < .001) and without a detectable change point. Other nodal factors, including nodal size, contralateral LN involvement (TNM stage N2c), and lower LN involvement (levels 4-5), were not associated with mortality in multivariable models when accounting for number of positive LNs. A novel, parsimonious nodal staging system derived by recursive partitioning analysis exhibited greater concordance with survival than the TNM staging system outlined in the American Joint Committee on Cancer's AJCC Staging Manual, 8th edition.
Conclusions and relevance: The number of metastatic nodes is a predominant independent factor associated with mortality in hypopharyngeal and laryngeal cancers. Moreover, standard nodal staging factors like LN size and contralaterality have no independent prognostic value when accounting for positive LN number. Deeper integration of quantitative metastatic nodal disease may simplify staging and better triage the need for adjuvant therapy.
Conflict of interest statement
Figures
Comment in
-
Characterizing an Ultra-High-Risk Subset of Patients With Hypopharynx and Larynx Cancer: The Power of Lymph Node Burden.JAMA Oncol. 2018 Jul 1;4(7):989-990. doi: 10.1001/jamaoncol.2017.3928. JAMA Oncol. 2018. PMID: 29192300 No abstract available.
References
-
- Lefebvre JL, Chevalier D, Luboinski B, Kirkpatrick A, Collette L, Sahmoud T; EORTC Head and Neck Cancer Cooperative Group . Larynx preservation in pyriform sinus cancer: preliminary results of a European Organization for Research and Treatment of Cancer phase III trial. J Natl Cancer Inst. 1996;88(13):890-899. - PubMed
-
- Pointreau Y, Garaud P, Chapet S, et al. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J Natl Cancer Inst. 2009;101(7):498-506. - PubMed
-
- Janoray G, Pointreau Y, Garaud P, et al. Long-term results of a multicenter randomized phase III trial of induction chemotherapy with cisplatin, 5-fluorouracil, ± docetaxel for larynx preservation. J Natl Cancer Inst. 2015;108(4):djv368. - PubMed
-
- Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349(22):2091-2098. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
