

Clinical Implementation of Pharmacogenetic Testing in a Hospital of the Spanish National Health System: Strategy and Experience Over 3 Years
- PMID: 29193749
- PMCID: PMC5866958
- DOI: 10.1111/cts.12526
Clinical Implementation of Pharmacogenetic Testing in a Hospital of the Spanish National Health System: Strategy and Experience Over 3 Years
Abstract
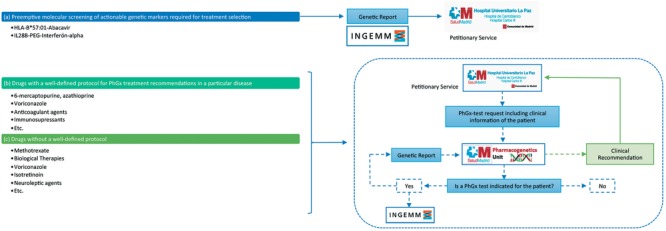
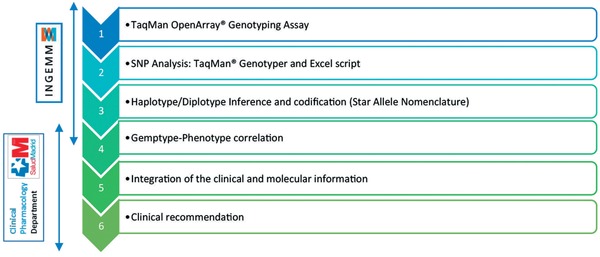
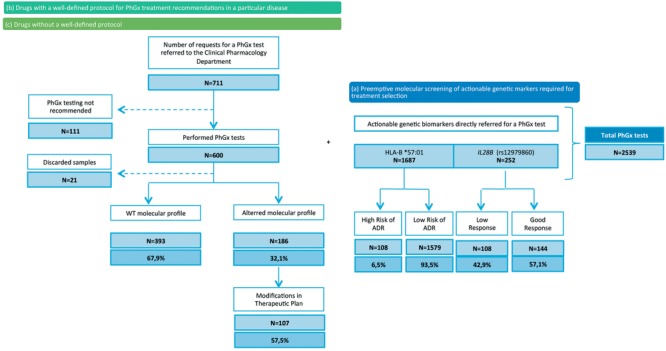
In 2014, we established a pharmacogenetics unit with the intention of facilitating the integration of pharmacogenetic testing into clinical practice. This unit was centered around two main ideas: i) individualization of clinical recommendations, and ii) preemptive genotyping in risk populations. Our unit is based on the design and validation of a single nucleotide polymorphism (SNP) microarray, which has allowed testing of 180 SNPs associated with drug response (PharmArray), and clinical consultation regarding the results. Herein, we report our experience in integrating pharmacogenetic testing into our hospital and we present the results of the 2,539 pharmacogenetic consultation requests received over the past 3 years in our unit. The results demonstrate the feasibility of implementing pharmacogenetic testing in clinical practice within a national health system.
Keywords: individualization; pharmacogenetics; precision medicine.
© 2017 The Authors. Clinical and Translational Science published by Wiley Periodicals, Inc. on behalf of American Society for Clinical Pharmacology and Therapeutics.
Figures
References
-
- International Conference on Harmonisation; guidance on specifications: test procedures and acceptance criteria for biotechnological/biological products. Notice. Food and Drug Administration, HHS. Fed. Regist. 64, 44928–44935 (1999). - PubMed
-
- Ehmann, F. et al Pharmacogenomic information in drug labels: European Medicines Agency perspective. Pharmacogenomics J. 15, 201–210 (2015). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
