

Bias in Radiology: The How and Why of Misses and Misinterpretations
- PMID: 29194009
- PMCID: PMC5790309
- DOI: 10.1148/rg.2018170107
Bias in Radiology: The How and Why of Misses and Misinterpretations
Abstract
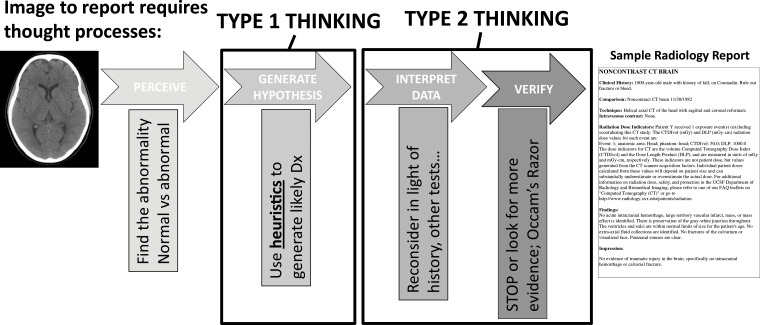
Medical errors are a leading cause of morbidity and mortality in the medical field and are substantial contributors to medical costs. Radiologists play an integral role in the diagnosis and care of patients and, given that those in this field interpret millions of examinations annually, may therefore contribute to diagnostic errors. Errors can be categorized as a "miss" when a primary or critical finding is not observed or as a "misinterpretation" when errors in interpretation lead to an incorrect diagnosis. In this article, the authors describe the cognitive causes of such errors in diagnostic medicine, specifically in radiology. Recognizing the cognitive processes that radiologists use while interpreting images should improve one's awareness of the inherent biases that can impact decision making. The authors review the common biases that impact clinical decisions, as well as strategies to counteract or minimize the potential for misdiagnosis. System-level processes that can be implemented to minimize cognitive errors are reviewed, as well as ways to implement personal changes to minimize cognitive errors in daily practice. ©RSNA, 2017.
Figures






References
-
- Kohn LT, Corrigan JM, Donaldson MS, et al. To err is human: building a safer health system. Washington, DC: National Academies Press, 2000. - PubMed
-
- Makary MA, Daniel M. Medical error: the third leading cause of death in the US. BMJ 2016;353:i2139. - PubMed
-
- Lee CS, Nagy PG, Weaver SJ, Newman-Toker DE. Cognitive and system factors contributing to diagnostic errors in radiology. AJR Am J Roentgenol 2013;201(3):611–617. - PubMed
-
- Berlin L. Malpractice issues in radiology: perceptual errors. AJR Am J Roentgenol 1996;167(3):587–590. - PubMed
-
- Garland LH. Studies on the accuracy of diagnostic procedures. Am J Roentgenol Radium Ther Nucl Med 1959;82(1):25–38. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
