

Cost-effectiveness Analysis of Intraoperative Cell Salvage for Obstetric Hemorrhage
- PMID: 29194062
- PMCID: PMC5771819
- DOI: 10.1097/ALN.0000000000001981
Cost-effectiveness Analysis of Intraoperative Cell Salvage for Obstetric Hemorrhage
Abstract
Background: Cost-effectiveness analyses on cell salvage for cesarean delivery to inform national and societal guidelines on obstetric blood management are lacking. This study examined the cost-effectiveness of cell salvage strategies in obstetric hemorrhage from a societal perspective.
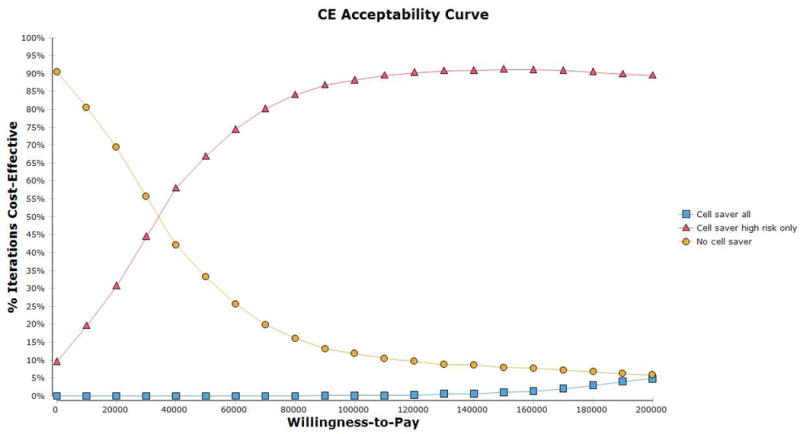
Methods: Markov decision analysis modeling compared the cost-effectiveness of three strategies: use of cell salvage for every cesarean delivery, cell salvage use for high-risk cases, and no cell salvage. A societal perspective and lifetime horizon was assumed for the base case of a 26-yr-old primiparous woman presenting for cesarean delivery. Each strategy integrated probabilities of hemorrhage, hysterectomy, transfusion reactions, emergency procedures, and cell salvage utilization; utilities for quality of life; and costs at the societal level. One-way and Monte Carlo probabilistic sensitivity analyses were performed. A threshold of $100,000 per quality-adjusted life-year gained was used as a cost-effectiveness criterion.
Results: Cell salvage use for cases at high risk for hemorrhage was cost-effective (incremental cost-effectiveness ratio, $34,881 per quality-adjusted life-year gained). Routine cell salvage use for all cesarean deliveries was not cost-effective, costing $415,488 per quality-adjusted life-year gained. Results were not sensitive to individual variation of other model parameters. The probabilistic sensitivity analysis showed that at the $100,000 per quality-adjusted life-year gained threshold, there is more than 85% likelihood that cell salvage use for cases at high risk for hemorrhage is favorable.
Conclusions: The use of cell salvage for cases at high risk for obstetric hemorrhage is economically reasonable; routine cell salvage use for all cesarean deliveries is not. These findings can inform the development of public policies such as guidelines on management of obstetric hemorrhage.
Conflict of interest statement
Figures


References
-
- The World Health Organization Fact Sheet No. 348: Maternal Mortality. Edited by Available from http://www.who.int/mediacentre/factsheets/fs348/en/. Accessed November 26, 2015.
-
- Goucher H, Wong CA, Patel SK, Toledo P. Cell Salvage in Obstetrics. Anesth Analg. 2015;121:465–8. - PubMed
-
- Waters JH. Indications and contraindications of cell salvage. Transfusion. 2004;44:40S–4S. - PubMed
-
- Allam J, Cox M, Yentis SM. Cell salvage in obstetrics. Int J Obstet Anesth. 2008;17:37–45. - PubMed
-
- Ashworth A, Klein AA. Cell salvage as part of a blood conservation strategy in anaesthesia. Br J Anaesth. 2010;105:401–16. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
