

Clinicopathologic Features and Prognostic Impact of Lymph Node Involvement in Patients With Breast Implant-associated Anaplastic Large Cell Lymphoma
- PMID: 29194092
- PMCID: PMC7500854
- DOI: 10.1097/PAS.0000000000000985
Clinicopathologic Features and Prognostic Impact of Lymph Node Involvement in Patients With Breast Implant-associated Anaplastic Large Cell Lymphoma
Abstract
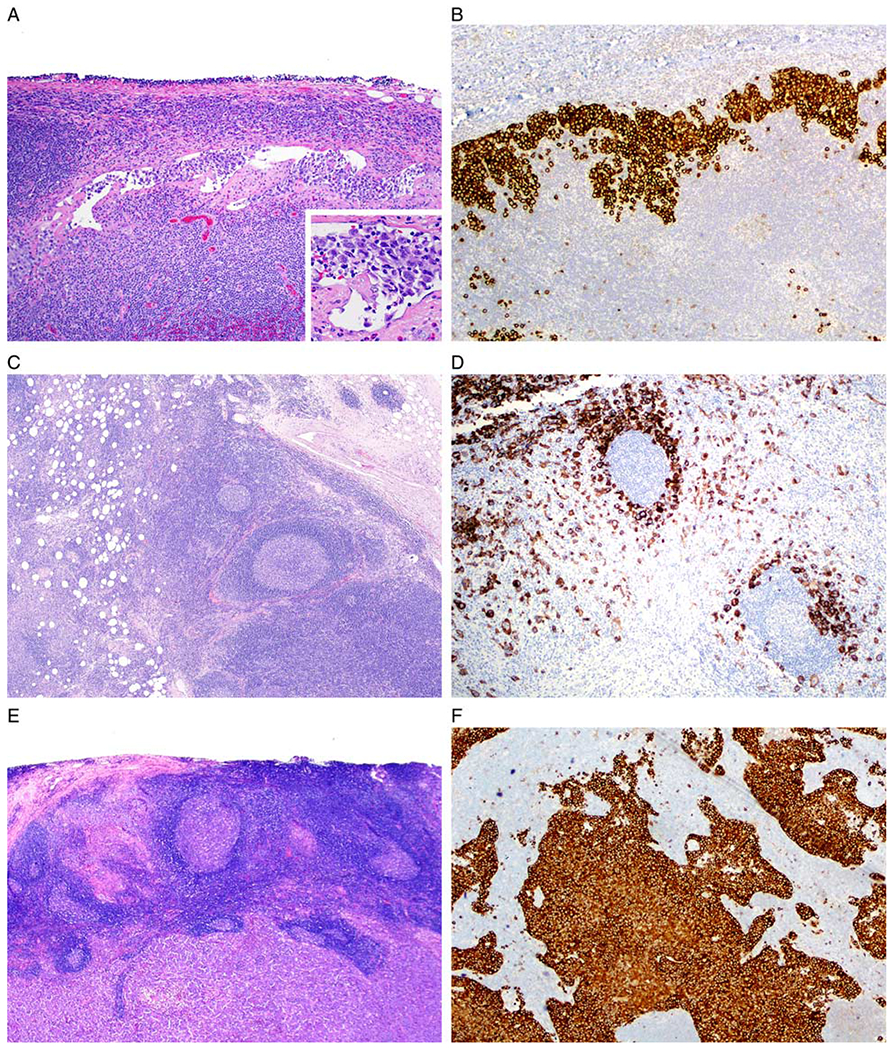
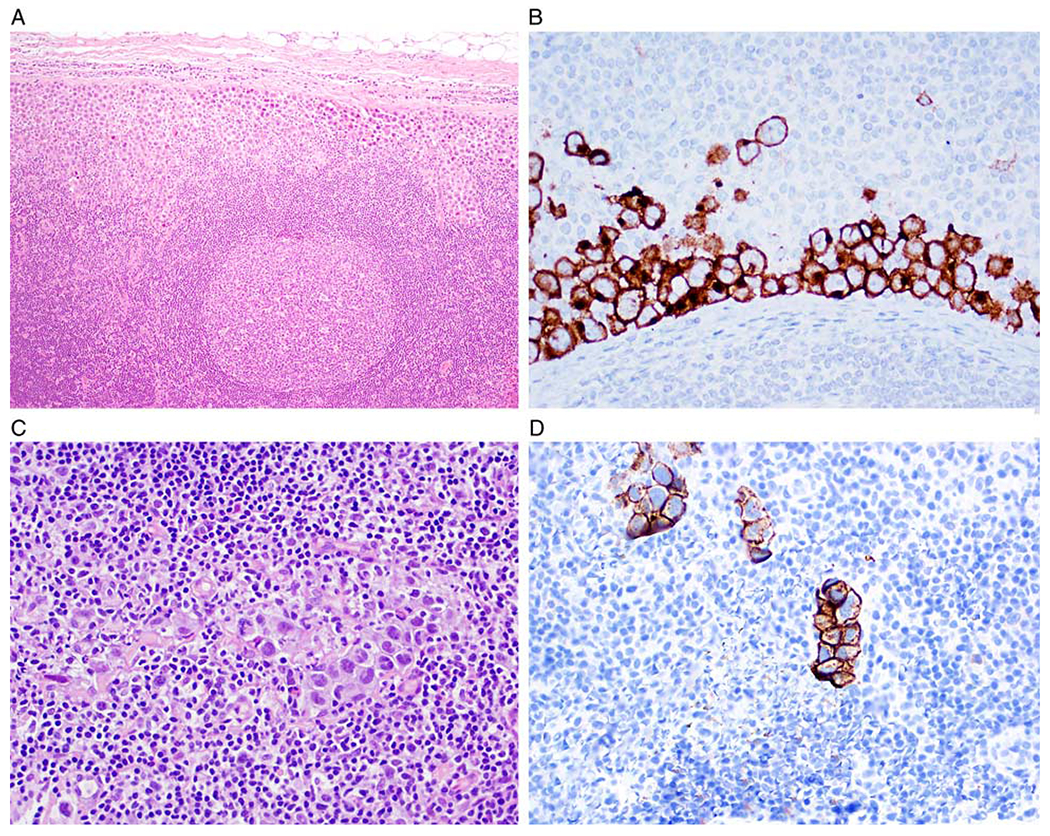
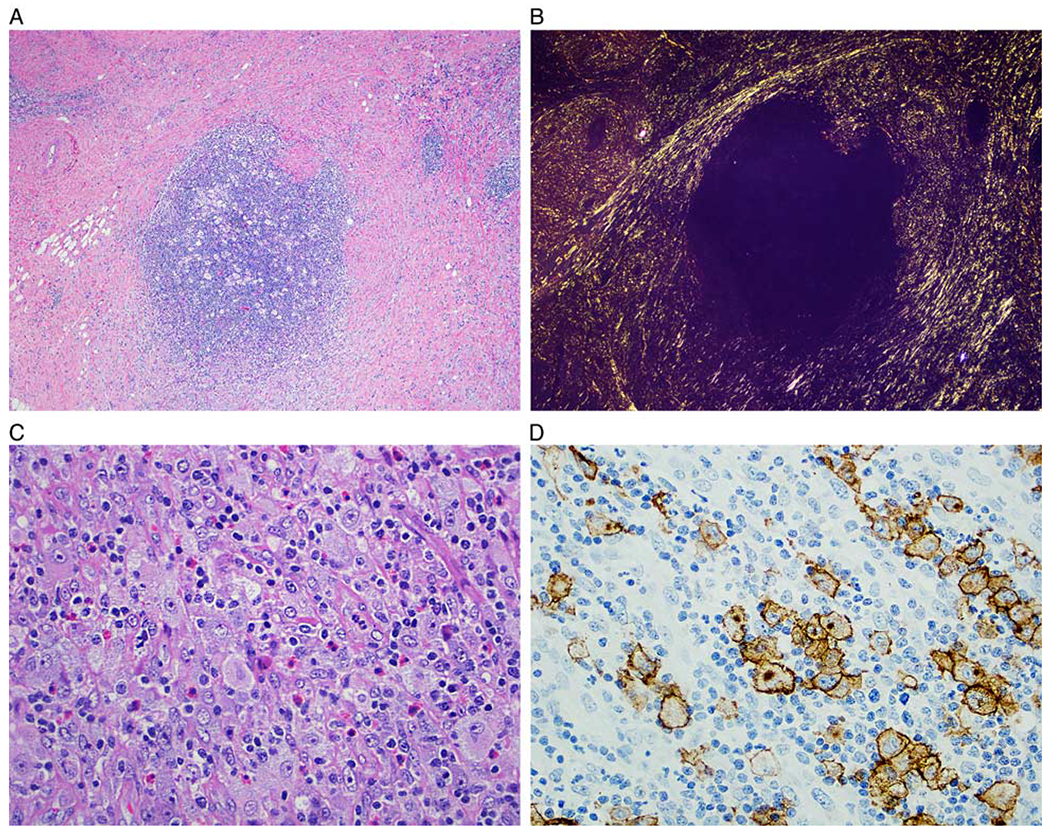
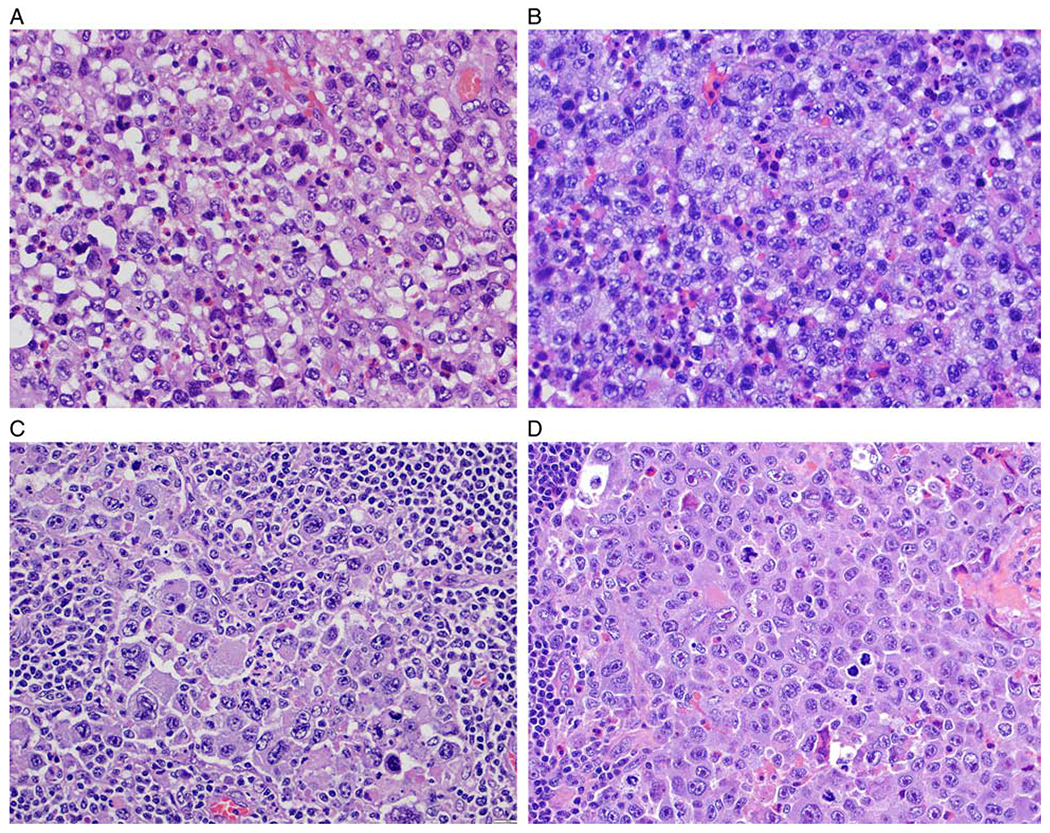
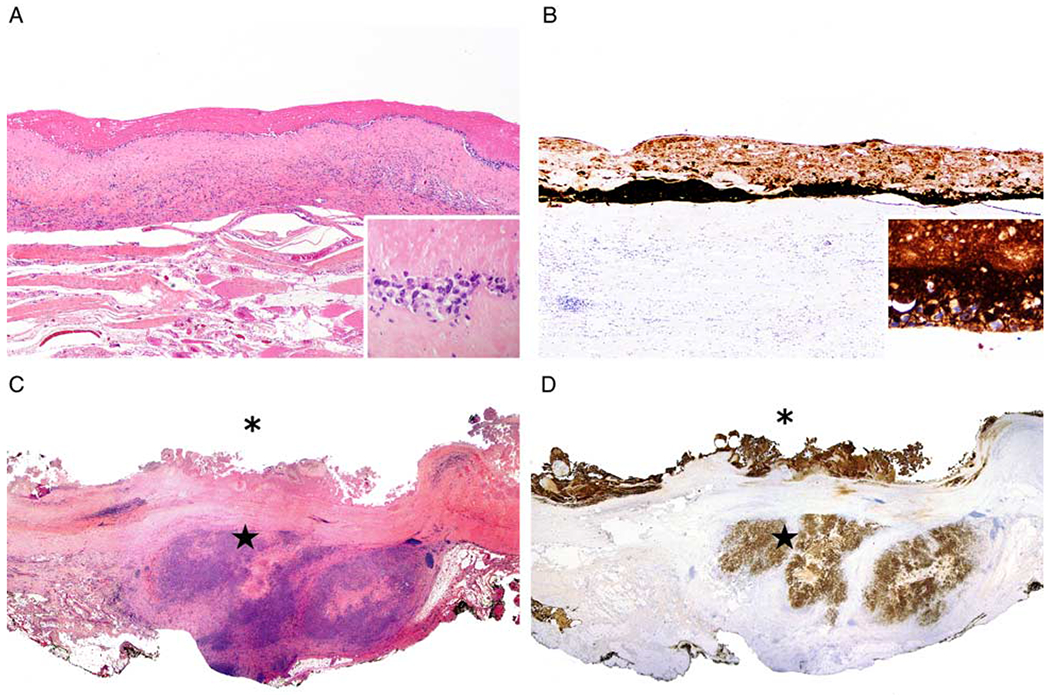
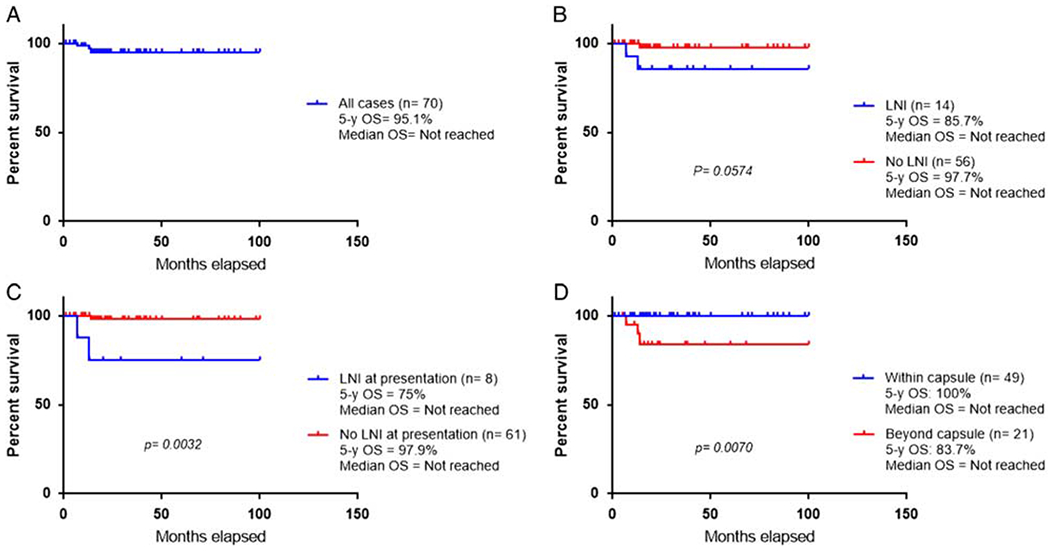
Breast implant-associated anaplastic large cell lymphoma (BI-ALCL) is a rare T-cell lymphoma that arises around breast implants. Most patients manifest with periprosthetic effusion, whereas a subset of patients develops a tumor mass or lymph node involvement (LNI). The aim of this study is to describe the pathologic features of lymph nodes from patients with BI-ALCL and assess the prognostic impact of LNI. Clinical findings and histopathologic features of lymph nodes were assessed in 70 patients with BI-ALCL. LNI was defined by the histologic demonstration of ALCL in lymph nodes. Fourteen (20%) patients with BI-ALCL had LNI, all lymph nodes involved were regional, the most frequent were axillary (93%). The pattern of involvement was sinusoidal in 13 (92.9%) cases, often associated with perifollicular, interfollicular, and diffuse patterns. Two cases had Hodgkin-like patterns. The 5-year overall survival was 75% for patients with LNI and 97.9% for patients without LNI at presentation (P=0.003). Six of 49 (12.2%) of patients with tumor confined by the capsule had LNI, compared with LNI in 8/21 (38%) patients with tumor beyond the capsule. Most patients with LNI achieved complete remission after various therapeutic approaches. Two of 14 (14.3%) patients with LNI died of disease compared with 0/56 (0%) patients without LNI. Twenty percent of patients with BI-ALCL had LNI by lymphoma, most often in a sinusoidal pattern. We conclude that BI-ALCL beyond capsule is associated with a higher risk of LNI. Involvement of lymph nodes was associated with decreased overall survival. Misdiagnosis as Hodgkin lymphoma is a pitfall.
Figures
References
-
- Keech JA Jr, Creech BJ. Anaplastic T-cell lymphoma in proximity to a saline-filled breast implant. Plast Reconstr Surg. 1997;100:554–555. - PubMed
-
- Miranda RM, Medeiros LJ. Breast implant-associated anaplastic large cell lymphoma In: Medeiros LJ, Miranda RN, eds. Diagnostic Pathology: Lymph Nodes and Extranodal Lymphomas. 2nd ed. Salt Lake City, UT: Elsevier; 2018:634–643.
-
- Doren EL, Miranda RN, Selber JC, et al. US epidemiology of breast implant-associated anaplastic large cell lymphoma. Plast Reconstr Surg. 2017;139:1042–1050. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
