

Risk Factors for the Development of Acute Respiratory Distress Syndrome Following Hemorrhage
- PMID: 29194339
- PMCID: PMC5976504
- DOI: 10.1097/SHK.0000000000001073
Risk Factors for the Development of Acute Respiratory Distress Syndrome Following Hemorrhage
Abstract
Background: The Pragmatic Randomized Optimal Platelet and Plasma Ratios (PROPPR) study evaluated the effects of plasma and platelets on hemostasis and mortality after hemorrhage. The pulmonary consequences of resuscitation strategies that mimic whole blood, remain unknown.
Methods: A secondary analysis of the PROPPR study was performed. Injured patients predicted to receive a massive transfusion were randomized to 1:1:1 versus 1:1:2 plasma-platelet-red blood cell ratios at 12 Level I North American trauma centers. Patients with survival >24 h, an intensive care unit (ICU) stay, and a recorded PaO2/FiO2 (P/F) ratio were included. Acute respiratory distress syndrome (ARDS) was defined as a P/F ratio < 200, with bilateral pulmonary infiltrates, and adjudicated by investigators.
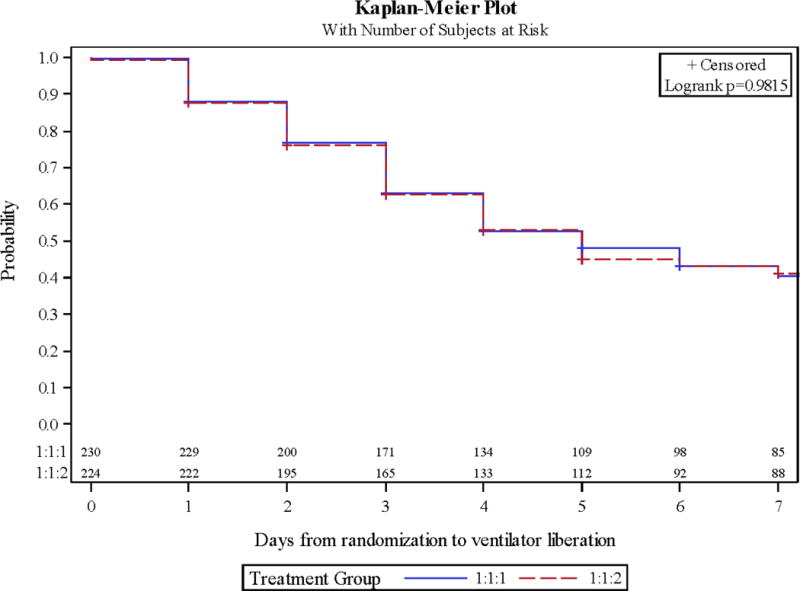
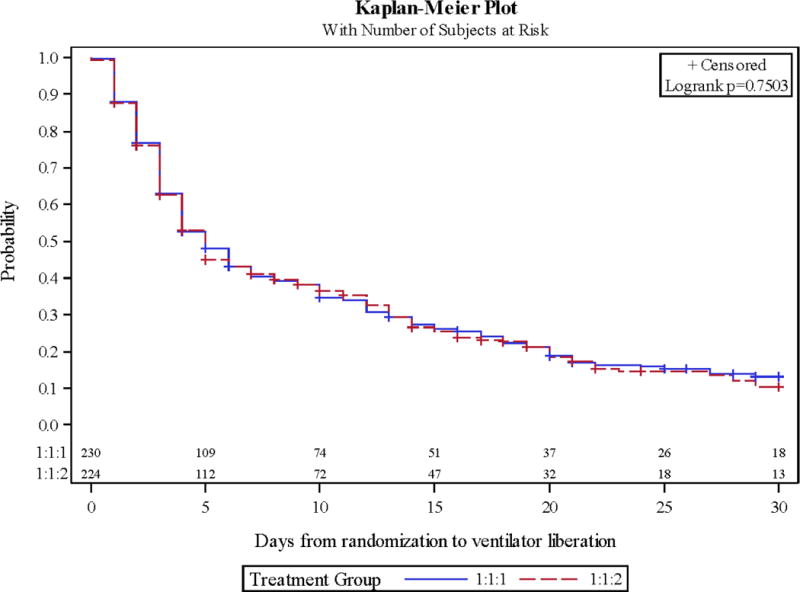
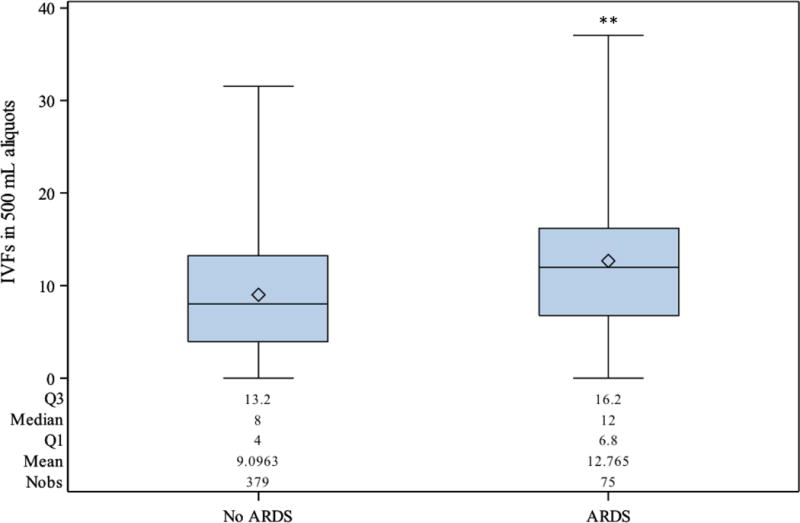
Results: Four hundred fifty-four patients were reviewed (230 received 1:1:1, 224 1:1:2). Age, sex, injury mechanism, and regional abbreviated injury scale (AIS) scores did not differ between cohorts. Tidal volume, positive end-expiratory pressure, and lowest P/F ratio did not differ. No significant differences in ARDS rates (14.8% vs. 18.4%), ventilator-free (24 vs. 24) or ICU-free days (17.5 vs. 18), hospital length of stay (22 days vs. 18 days), or 30-day mortality were found (28% vs. 28%). ARDS was associated with blunt injury (OR 3.61 [1.53-8.81] P < 0.01) and increasing chest AIS (OR 1.40 [1.15-1.71] P < 0.01). Each 500 mL of crystalloid infused during hours 0 to 6 was associated with a 9% increase in the rate of ARDS (OR 1.09 [1.04-1.14] P < 0.01). Blood given at 0 to 6 or 7 to 24 h were not risk factors for lung injury.
Conclusion: Acute crystalloid exposure, but not blood products, is a potentially modifiable risk factor for the prevention of ARDS following hemorrhage.
Conflict of interest statement
Mr. Branson reports relationships with the following companies: Mallinckrodt
Ventec Life Systems, Meiji Pharmaceuticals, Bayer, MedPace, Medtronic, and Ciel Medical
Figures
References
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet. 1967;2:319–323. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA. 2016;315:788–800. - PubMed
-
- ARDS Definition Task Force. Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–2533. - PubMed
-
- Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med. 1995;151:293–301. - PubMed
-
- Miller PR, Croce MA, Kilgo PD, Scott J, Fabian TC. Acute respiratory distress syndrome in blunt trauma: identification of independent risk factors. Am Surg. 2002;68:1. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
