

Bleeding complications in acute liver failure
- PMID: 29194678
- PMCID: PMC5906191
- DOI: 10.1002/hep.29694
Bleeding complications in acute liver failure
Abstract
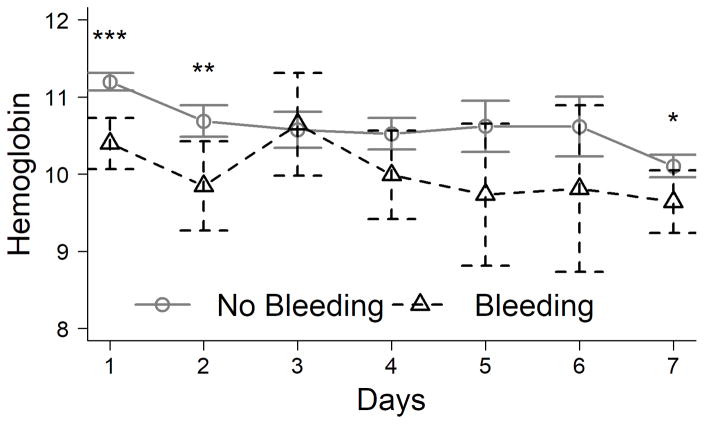
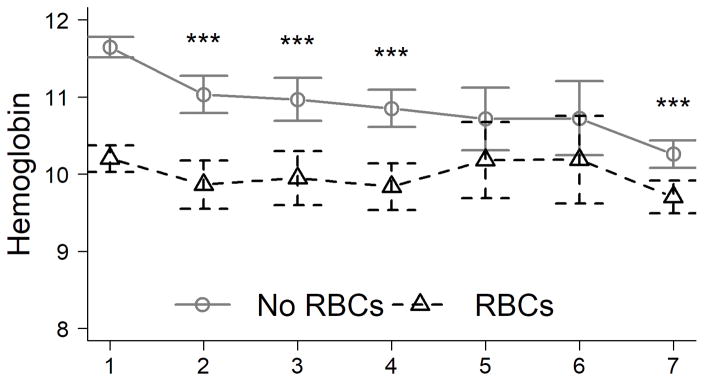
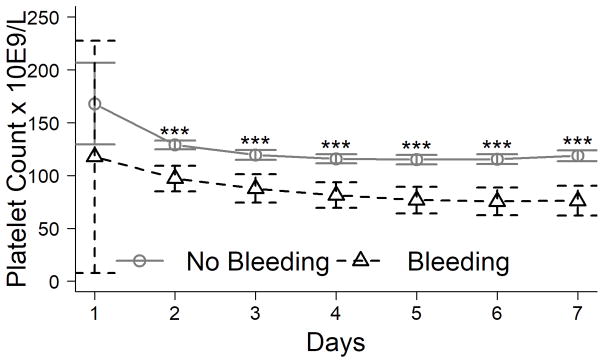
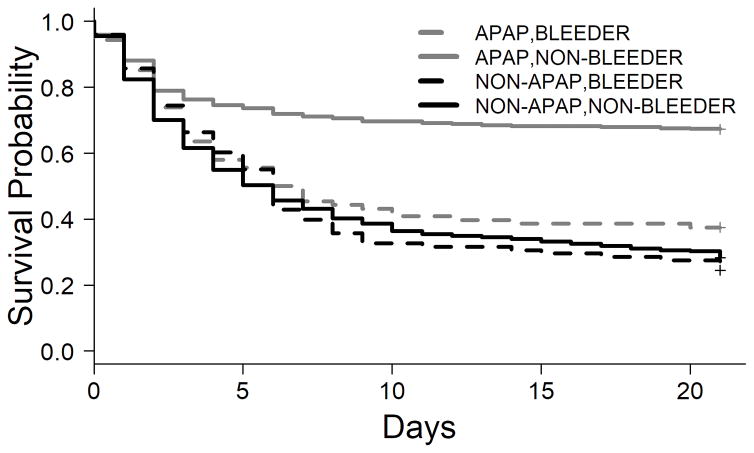
In patients with acute liver failure (ALF), elevated prothrombin time and thrombocytopenia can fuel a perception of a bleeding tendency. However, the incidence, site, risk factors, and clinical significance of bleeding complications have not been quantified in a large cohort of patients with ALF. We studied 1,770 adult patients enrolled in the ALF Study Group Registry between 1998 and 2016. Bleeding complications and blood component transfusions were collected for 7 days after admission. The relationship of bleeding complications to 21-day mortality was assessed. Despite a median international normalized ratio of 2.7 and platelet count of 96 × 109 /L on admission, bleeding complications were observed in only 187 patients (11%), including 173 spontaneous and 22 postprocedural bleeding episodes. Eighty-four percent of spontaneous bleeding episodes were from an upper gastrointestinal source and rarely resulted in red blood cell transfusion. Twenty patients experienced an intracranial bleed; half of these occurred spontaneously and half after intracranial pressure monitor placement, and this was the proximate cause of death in 20% and 50%, respectively. Bleeders and patients who received red blood cell transfusions were more acutely ill from extrahepatic organ system failure but not from hepatocellular failure. Consistent with this observation, bleeding complications were associated with lower platelet counts but not higher international normalized ratio. Transfusion of any blood component was associated with nearly 2-fold increased death or need for liver transplantation at day 21, but bleeding complications were the proximate cause of death in only 5% of cases.
Conclusions: Despite a perceived bleeding diathesis, clinically significant bleeding is uncommon in patients with ALF; bleeding complications in patients with ALF are markers of severe systemic inflammation rather than of coagulopathy and so portend a poor prognosis. (Hepatology 2018;67:1931-1942).
© 2017 by the American Association for the Study of Liver Diseases.
Figures

References
-
- Trey C, Davidson CS. The management of fulminant hepatic failure. Prog Liver Dis. 1970;3:282–298. - PubMed
-
- Agarwal B, Wright G, Gatt A, Riddell A, Vemala V, Mallett S, et al. Evaluation of coagulation abnormalities in acute liver failure. J Hepatol. 2012;57:780–786. - PubMed
-
- Lisman T, Stravitz RT. Rebalanced Hemostasis in Patients with Acute Liver Failure. Semin Thromb Hemost. 2015;41:468–473. - PubMed
-
- Ritt DJ, Whelan G, Werner DJ, Eigenbrodt EH, Schenker S, Combes B. Acute hepatic necrosis with stupor or coma. An analysis of thirty-one patients. Medicine (Baltimore) 1969;48:151–172. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
