

Type 2 diabetes mellitus is associated with a lower fibrous cap thickness but has no impact on calcification morphology: an intracoronary optical coherence tomography study
- PMID: 29195505
- PMCID: PMC5709861
- DOI: 10.1186/s12933-017-0635-2
Type 2 diabetes mellitus is associated with a lower fibrous cap thickness but has no impact on calcification morphology: an intracoronary optical coherence tomography study
Abstract
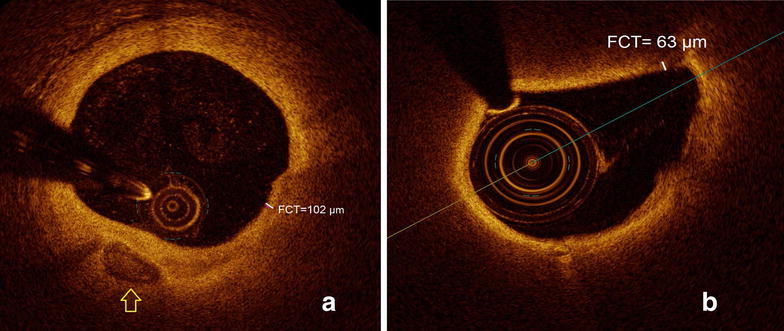
Background: Patients with type 2 diabetes (T2DM) are at high risk for cardiovascular events, which usually arise from the rupture of a vulnerable coronary plaque. The minimal fibrous cap thickness (FCT) overlying a necrotic lipid core is an established predictor for plaque rupture. Recently, coronary calcification has emerged as a relevant feature of plaque vulnerability. However, the impact of T2DM on these morphological plaque parameters is largely unexplored. Therefore, this study aimed to compare differences of coronary plaque morphology in patients with and without T2DM with a particular focus on coronary calcification.
Methods: In 91 patients (T2DM = 56, non-T2DM = 35) with 105 coronary de novo lesions (T2DM = 56, non-T2DM = 49) plaque morphology and calcification were analyzed using optical coherence tomography (OCT) prior to coronary intervention.
Results: Patients with T2DM had a lower minimal FCT (80.4 ± 27.0 µm vs. 106.8 ± 27.8 µm, p < 0.001) and a higher percent area stenosis (77.9 ± 8.1% vs. 71.7 ± 11.2%, p = 0.001) compared to non-diabetic subjects. However, patients with and without T2DM had a similar total number of calcifications (4.0 ± 2.6 vs. 4.2 ± 3.1, p = ns) and no significant difference was detected in the number of micro- (0.34 ± 0.79 vs. 0.31 ± 0.71), spotty (2.11 ± 1.77 vs. 2.37 ± 1.89) or macro-calcifications (1.55 ± 1.13 vs. 1.53 ± 0.71, all p = ns). The mean calcium arc (82.3 ± 44.8° vs. 73.7 ± 31.6), the mean thickness of calcification (0.54 ± 0.13 mm vs. 0.51 ± 0.15 mm), the mean calcified area (0.99 ± 0.72 mm2 vs. 0.78 ± 0.49 mm2), the mean depth of calcification (172 ± 192 μm vs. 160 ± 76 μm) and the cap thickness overlying the calcification (50 ± 71 μm vs. 62 ± 61 μm) did not differ between the diabetic and non-diabetic groups (all p = ns).
Conclusion: T2DM has an impact on the minimal FCT of the coronary target lesion, but not on localization, size, shape or extent of calcification. Thus, the minimal FCT overlying the necrotic lipid core but not calcification is likely to contribute to the increased plaque vulnerability observed in patients with T2DM.
Keywords: Coronary calcification; Diabetes mellitus; Optical coherence tomography; Plaque vulnerability.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
