

Meta-Analysis of the Safety and Efficacy of the Oral Anticoagulant Agents (Apixaban, Rivaroxaban, Dabigatran) in Patients With Acute Coronary Syndrome
- PMID: 29195825
- PMCID: PMC7453967
- DOI: 10.1016/j.amjcard.2017.10.035
Meta-Analysis of the Safety and Efficacy of the Oral Anticoagulant Agents (Apixaban, Rivaroxaban, Dabigatran) in Patients With Acute Coronary Syndrome
Abstract
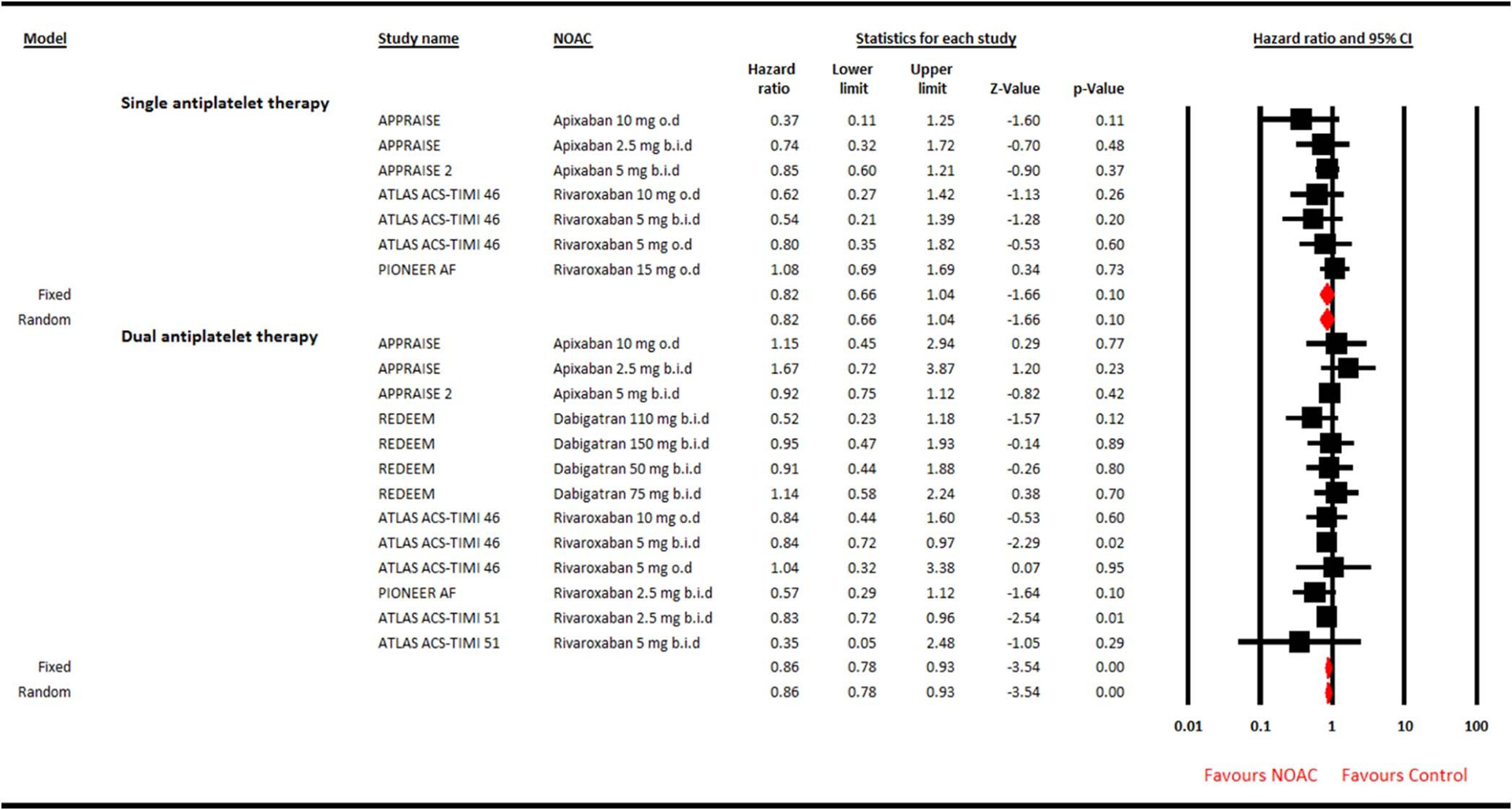
The significance of adding new oral anticoagulants (NOACs) to antiplatelet therapy in patients with acute coronary syndrome (ACS) is unclear. We conducted a meta-analysis to assess the safety and efficacy of adding NOACs (apixaban, rivaroxaban, and dabigatran) to single antiplatelet agent (SAP) or dual antiplatelet therapy (DAPT) in patients with ACS. Seven randomized controlled trials were selected using PubMed or MEDLINE, Scopus, and Cochrane library (inception to August 2017). The summary measure was random effects hazard ratio (HR) with 95% confidence interval (CI). The primary safety outcome was clinically significant bleeding. The secondary efficacy outcome was major adverse cardiovascular events (MACE; composite of myocardial infarction, stroke, and all-cause mortality). In 31,574 patients, addition of NOAC to SAP did not increase the risk of clinically significant bleeding (HR 0.82, 95% CI 0.56 to 1.20, p = 0.31); however, the risk of clinically significant bleeding was significantly increased with NOAC plus DAPT (HR 2.24, 95% CI 1.75 to 2.87, p < 0.001). NOACs had no statistically beneficial effect on MACE when used with SAP (HR 0.82, 95% CI 0.66 to 1.04, p = 0.10); however, a modest reduction in MACE was observed when NOACs were combined with DAPT (HR 0.86, 95% CI 0.78 to 0.93, p < 0.001). In conclusion, in patients with ACS, the addition of NOAC to DAPT resulted in increased risk of clinically significant bleeding, whereas only a modest reduction in MACE was achieved. The addition of NOACs to SAP did not result in significant reduction of MACE or increase in clinically significant bleeding.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures


References
-
- Paravattil B, Elewa H. Strategies to optimize dual antiplatelet therapy after coronary artery stenting in acute coronary syndrome. J Cardiovasc Pharmacol Ther 2017;22:347–355. - PubMed
-
- Libby P Mechanisms of acute coronary syndromes. N Engl J Med 2013;369:883–884. - PubMed
-
- Monroe DM, Hoffman M, Roberts HR. Platelets and thrombin generation. Arterioscler Thromb Vasc Biol 2002;22:1381–1389. - PubMed
-
- Hurlen M, Abdelnoor M, Smith P, Erikssen J, Arnesen H. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med 2002;347:969–974. - PubMed
-
- van Es RF, Jonker JJ, Verheugt FW, Deckers JW, Grobbee DE. Aspirin and coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet 2002;360:109–113. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
