

Rubella vaccination in India: identifying broad consequences of vaccine introduction and key knowledge gaps
- PMID: 29198212
- PMCID: PMC6024169
- DOI: 10.1017/S0950268817002527
Rubella vaccination in India: identifying broad consequences of vaccine introduction and key knowledge gaps
Abstract
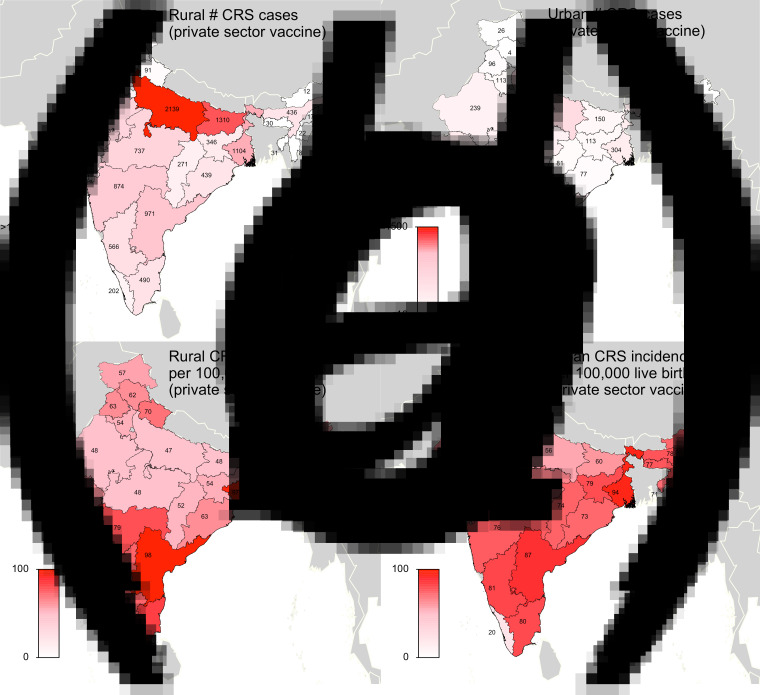
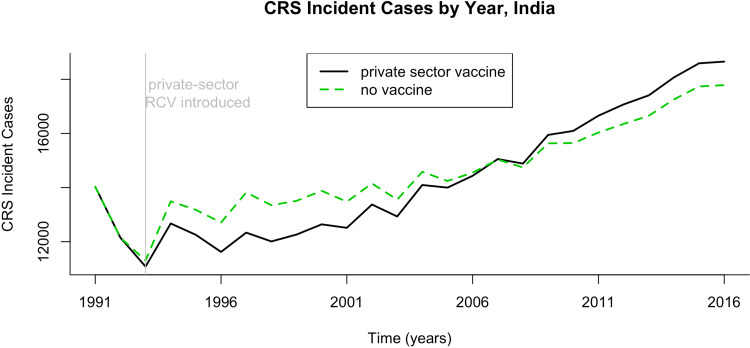
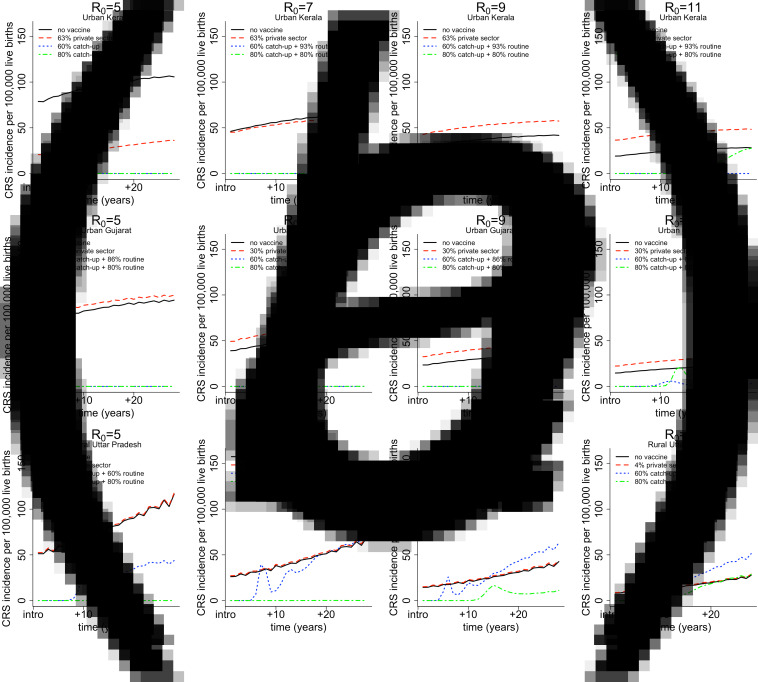
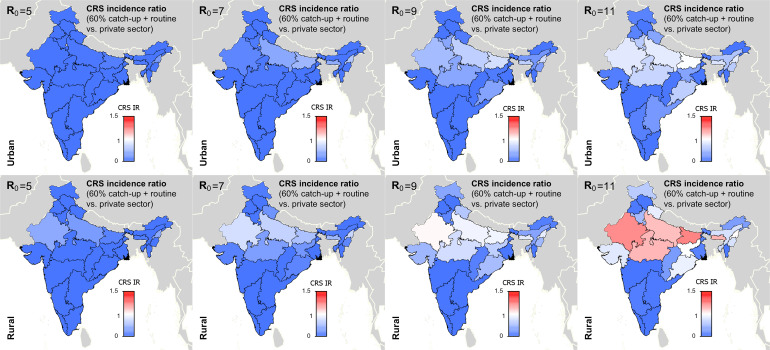
Rubella virus infection typically presents as a mild illness in children; however, infection during pregnancy may cause the birth of an infant with congenital rubella syndrome (CRS). As of February 2017, India began introducing rubella-containing vaccine (RCV) into the public-sector childhood vaccination programme. Low-level RCV coverage among children over several years can result in an increase in CRS incidence by increasing the average age of infection without sufficiently reducing rubella incidence. We evaluated the impact of RCV introduction on CRS incidence across India's heterogeneous demographic and epidemiological contexts. We used a deterministic age-structured model that reflects Indian states' rural and urban area-specific demography and vaccination coverage levels to simulate rubella dynamics and estimate CRS incidence with and without RCV introduction to the public sector. Our analysis suggests that current low-level private-sector vaccination has already slightly increased the burden of CRS in India. We additionally found that the effect of public-sector RCV introduction depends on the basic reproductive number, R 0, of rubella. If R 0 is five, a value empirically estimated from an array of settings, CRS incidence post-RCV introduction will likely decrease. However, if R 0 is seven or nine, some states may experience short-term or annual increases in CRS, even if a long-term total reduction in cases (30 years) is expected. Investment in population-based serological surveys and India's fever/rash surveillance system will be key to monitoring the success of the vaccination programme.
Keywords: CRS; Congenital rubella syndrome; India; rubella; vaccine.
Conflict of interest statement
None.
Figures

Similar articles
-
Progress Toward Rubella and Congenital Rubella Syndrome Control - South-East Asia Region, 2000-2016.MMWR Morb Mortal Wkly Rep. 2018 Jun 1;67(21):602-606. doi: 10.15585/mmwr.mm6721a3. MMWR Morb Mortal Wkly Rep. 2018. PMID: 29851943 Free PMC article.
-
Rubella immunity among pregnant women and the burden of congenital rubella syndrome (CRS) in India, 2022.Vaccine. 2024 Oct 24;42(24):126077. doi: 10.1016/j.vaccine.2024.06.044. Epub 2024 Jul 2. Vaccine. 2024. PMID: 38960788
-
Progress toward control of rubella and prevention of congenital rubella syndrome --- worldwide, 2009.MMWR Morb Mortal Wkly Rep. 2010 Oct 15;59(40):1307-10. MMWR Morb Mortal Wkly Rep. 2010. PMID: 20948509
-
Targeting rubella for elimination.Indian J Public Health. 2012 Oct-Dec;56(4):269-72. doi: 10.4103/0019-557X.106413. Indian J Public Health. 2012. PMID: 23354136 Review.
-
Congenital rubella syndrome: a matter of concern.Rev Panam Salud Publica. 2015 Mar;37(3):179-86. Rev Panam Salud Publica. 2015. PMID: 25988255 Review.
Cited by
-
The Impact of Rubella Vaccine Introduction on Rubella Infection and Congenital Rubella Syndrome: A Systematic Review of Mathematical Modelling Studies.Vaccines (Basel). 2021 Jan 25;9(2):84. doi: 10.3390/vaccines9020084. Vaccines (Basel). 2021. PMID: 33503898 Free PMC article.
-
Phylogeography of rubella virus in Asia: Vaccination and demography shape synchronous outbreaks.Epidemics. 2019 Sep;28:100346. doi: 10.1016/j.epidem.2019.100346. Epub 2019 May 28. Epidemics. 2019. PMID: 31201039 Free PMC article.
-
A review of safety and immunogenicity of a novel measles, mumps, rubella (MMR) vaccine.Hum Vaccin Immunother. 2024 Dec 31;20(1):2302685. doi: 10.1080/21645515.2024.2302685. Epub 2024 Jan 18. Hum Vaccin Immunother. 2024. PMID: 38236022 Free PMC article. Review.
-
Using models to shape measles control and elimination strategies in low- and middle-income countries: A review of recent applications.Vaccine. 2020 Jan 29;38(5):979-992. doi: 10.1016/j.vaccine.2019.11.020. Epub 2019 Nov 29. Vaccine. 2020. PMID: 31787412 Free PMC article. Review.
-
A Study Prevalence of Congenital Rubella Syndrome Cases Before and After Rubella Vaccination Campaign.Indian J Otolaryngol Head Neck Surg. 2023 Dec;75(4):2913-2920. doi: 10.1007/s12070-023-03882-3. Epub 2023 May 25. Indian J Otolaryngol Head Neck Surg. 2023. PMID: 37974742 Free PMC article.
References
-
- Miller E, Cradockwatson JE, Pollock TM. Consequences of confirmed maternal rubella at successive stages of pregnancy. Lancet 1982; 2: 781–784. - PubMed
-
- Reef S, Plotkin S. Rubella vaccines. In: Plotkin S, Orenstein W, Offit P, eds. Vaccines, 6th edn. Philadelphia, PA: Elsevier, 2013, pp. 688–717, chapter 31.
-
- Figueroa P, et al. XXII technical advisory group on Vaccine-Preventable Diseases (TAG) meeting. Technical report, Pan American Health Organization (PAHO), Washington, DC, 2014.
-
- Ministry of Women and Child Development, Government of India. Rapid Survey on Children (2013–14): India and state fact sheets, 2016 (http://wcd.nic.in/acts/rapid-survey-children-rsoc-2013-14). Accessed 4 January 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
