

Visualization Improves Supraclavicular Access to the Subclavian Vein in a Mixed Reality Simulator
- PMID: 29200069
- PMCID: PMC6774241
- DOI: 10.1213/ANE.0000000000002572
Visualization Improves Supraclavicular Access to the Subclavian Vein in a Mixed Reality Simulator
Abstract
Background: We investigated whether visual augmentation (3D, real-time, color visualization) of a procedural simulator improved performance during training in the supraclavicular approach to the subclavian vein, not as widely known or used as its infraclavicular counterpart.
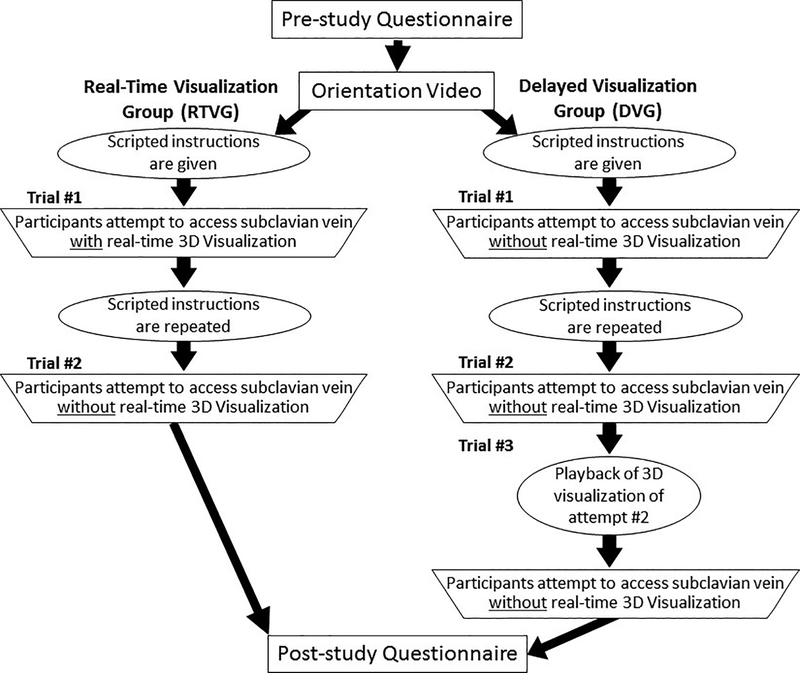
Methods: To train anesthesiology residents to access a central vein, a mixed reality simulator with emulated ultrasound imaging was created using an anatomically authentic, 3D-printed, physical mannequin based on a computed tomographic scan of an actual human. The simulator has a corresponding 3D virtual model of the neck and upper chest anatomy. Hand-held instruments such as a needle, an ultrasound probe, and a virtual camera controller are directly manipulated by the trainee and tracked and recorded with submillimeter resolution via miniature, 6 degrees of freedom magnetic sensors. After Institutional Review Board approval, 69 anesthesiology residents and faculty were enrolled and received scripted instructions on how to perform subclavian venous access using the supraclavicular approach based on anatomic landmarks. The volunteers were randomized into 2 cohorts. The first used real-time 3D visualization concurrently with trial 1, but not during trial 2. The second did not use real-time 3D visualization concurrently with trial 1 or 2. However, after trial 2, they observed a 3D visualization playback of trial 2 before performing trial 3 without visualization. An automated scoring system based on time, success, and errors/complications generated objective performance scores. Nonparametric statistical methods were used to compare the scores between subsequent trials, differences between groups (real-time visualization versus no visualization versus delayed visualization), and improvement in scores between trials within groups.
Results: Although the real-time visualization group demonstrated significantly better performance than the delayed visualization group on trial 1 (P = .01), there was no difference in gain scores, between performance on the first trial and performance on the final trial, that were dependent on group (P = .13). In the delayed visualization group, the difference in performance between trial 1 and trial 2 was not significant (P = .09); reviewing performance on trial 2 before trial 3 resulted in improved performance when compared to trial 1 (P < .0001). There was no significant difference in median scores (P = .13) between the real-time visualization and delayed visualization groups for the last trial after both groups had received visualization. Participants reported a significant improvement in confidence in performing supraclavicular access to the subclavian vein. Standard deviations of scores, a measure of performance variability, decreased in the delayed visualization group after viewing the visualization.
Conclusions: Real-time visual augmentation (3D visualization) in the mixed reality simulator improved performance during supraclavicular access to the subclavian vein. No difference was seen in the final trial of the group that received real-time visualization compared to the group that had delayed visualization playback of their prior attempt. Training with the mixed reality simulator improved participant confidence in performing an unfamiliar technique.
Conflict of interest statement
Conflict of interest: No conflicts of interest.
Figures

Comment in
-
New Technology, New Thinking.Anesth Analg. 2018 Jul;127(1):7-8. doi: 10.1213/ANE.0000000000003332. Anesth Analg. 2018. PMID: 29912052 No abstract available.
References
-
- Yoffa D. Supraclavicular subclavian venepuncture and catheterisation. Lancet. 1965;2:614–617. - PubMed
-
- Conroy JM, Rajagopalan PR, Baker JD, Bailey MK. A modification of the supraclavicular approach to the central circulation. South Med J. 1990;83:1178–1181. - PubMed
-
- Dronen S, Thompson B, Nowak R, Tomlanovich M. Subclavian vein catheterization during cardiopulmonary resuscitation. A prospective comparison of the supraclavicular and infraclavicular percutaneous approaches. JAMA. 1982;247:3227–3230. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
