

Serologic Response to Treatment in Human Immunodeficiency Virus-Negative Syphilis Patients Using Automated Serological Tests: Proposals for New Guidelines
- PMID: 29200767
- PMCID: PMC5705360
- DOI: 10.5021/ad.2017.29.6.768
Serologic Response to Treatment in Human Immunodeficiency Virus-Negative Syphilis Patients Using Automated Serological Tests: Proposals for New Guidelines
Abstract
Background: Automated analyzer-based nontreponemal serological tests for syphilis (STS) have been used for several decades.
Objective: In this study, we evaluated serological responses to treatment and proposed clinical guidelines for automated STS.
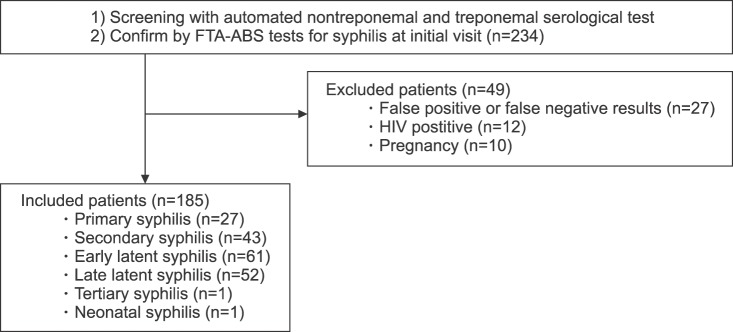
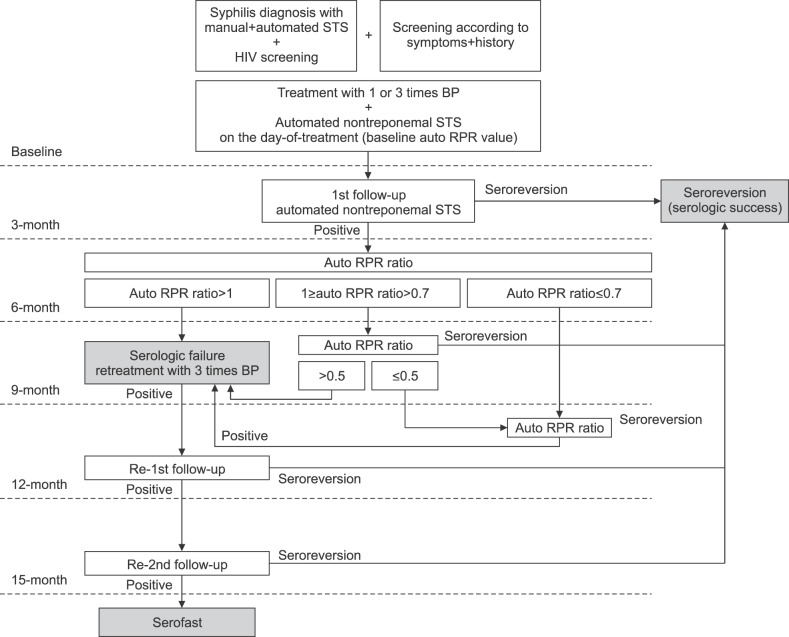
Methods: This retrospective cohort study analyzed human immunodeficiency virus-negative syphilis patients who were diagnosed with automated rapid plasma reagin (auto RPR) tests as a nontreponemal STS, and who also received the fluorescent treponemal antibody-absorption test as a confirmatory test. The ratio of auto RPR values after treatment against those at baseline was defined as the auto RPR ratio for the analysis of the serological response to treatment. The cutoff value for reliable seroreversion prediction was assessed with receiver-operating-characteristic curves.
Results: Overall, 89.7% of participants (78/87) seroreverted and 10.3% of participants (9/87) remained serofast during the two-year follow-up period. We were unable to describe trends in the changes among auto RPR values within six months after treatment because of high variation. All of the patients who had an auto RPR ratio ≥1.0 after six months continuously had positive serologic results during their 24-month follow-up and were classified as a serofast group. The receiver-operating-characteristic curves revealed a 25% reduction in auto RPR values nine months after treatment and predicted seroreversion with a sensitivity of 96.2% and a specificity of 100%.
Conclusion: The most important primary checkpoint for syphilis treatment response is an increase in automated nontreponemal STS six months after treatment. Thus, we recommend monitoring the treatment response with an auto RPR.
Keywords: Nontreponemal antibody test; Sexually transmitted diseases; Syphilis; Syphilis serodiagnosis; Treponema pallidum.
Conflict of interest statement
CONFLICTS OF INTEREST: The authors have nothing to disclose.
Figures
References
-
- Kampmeier RH. The introduction of penicillin for the treatment of syphilis. Sex Transm Dis. 1981;8:260–265. - PubMed
-
- Workowski KA, Berman S Centers for Disease Control and Prevention (CDC) Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59:1–110. - PubMed
-
- Janier M, Hegyi V, Dupin N, Unemo M, Tiplica GS, Potočnik M, et al. 2014 European guideline on the management of syphilis. J Eur Acad Dermatol Venereol. 2014;28:1581–1593. - PubMed
-
- Brown ST, Zaidi A, Larsen SA, Reynolds GH. Serological response to syphilis treatment. A new analysis of old data. JAMA. 1985;253:1296–1299. - PubMed
-
- Müller I, Brade V, Hagedorn HJ, Straube E, Schörner C, Frosch M, et al. Is serological testing a reliable tool in laboratory diagnosis of syphilis? Meta-analysis of eight external quality control surveys performed by the german infection serology proficiency testing program. J Clin Microbiol. 2006;44:1335–1341. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
