

Multivariable prediction model for suspected giant cell arteritis: development and validation
- PMID: 29200816
- PMCID: PMC5703153
- DOI: 10.2147/OPTH.S151385
Multivariable prediction model for suspected giant cell arteritis: development and validation
Abstract
Purpose: To develop and validate a diagnostic prediction model for patients with suspected giant cell arteritis (GCA).
Methods: A retrospective review of records of consecutive adult patients undergoing temporal artery biopsy (TABx) for suspected GCA was conducted at seven university centers. The pathologic diagnosis was considered the final diagnosis. The predictor variables were age, gender, new onset headache, clinical temporal artery abnormality, jaw claudication, ischemic vision loss (VL), diplopia, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and platelet level. Multiple imputation was performed for missing data. Logistic regression was used to compare our models with the non-histologic American College of Rheumatology (ACR) GCA classification criteria. Internal validation was performed with 10-fold cross validation and bootstrap techniques. External validation was performed by geographic site.
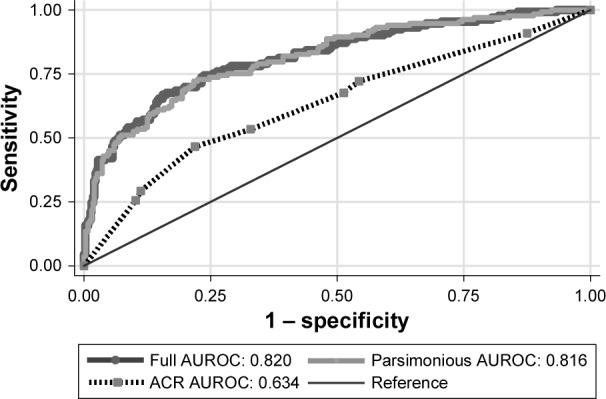
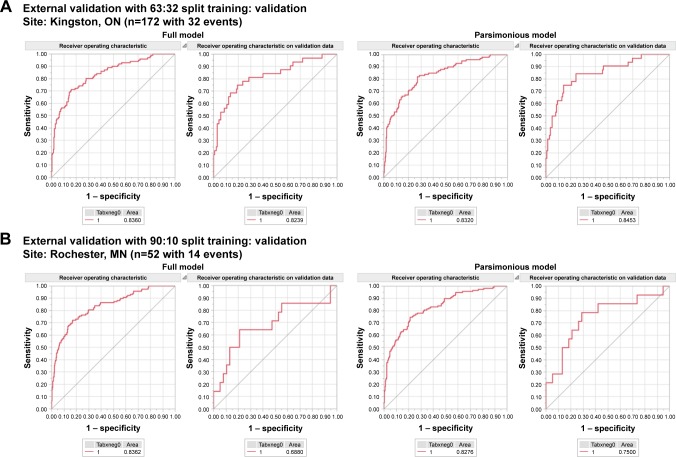
Results: There were 530 complete TABx records: 397 were negative and 133 positive for GCA. Age, jaw claudication, VL, platelets, and log CRP were statistically significant predictors of positive TABx, whereas ESR, gender, headache, and temporal artery abnormality were not. The parsimonious model had a cross-validated bootstrap area under the receiver operating characteristic curve (AUROC) of 0.810 (95% CI =0.766-0.854), geographic external validation AUROC's in the range of 0.75-0.85, calibration pH-L of 0.812, sensitivity of 43.6%, and specificity of 95.2%, which outperformed the ACR criteria.
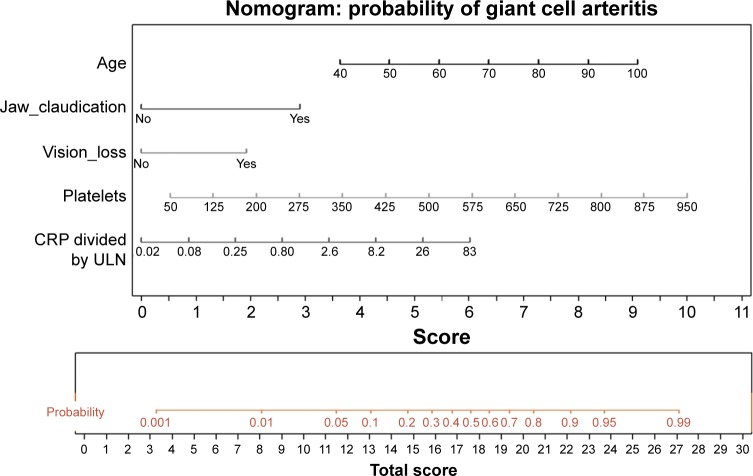
Conclusion: Our prediction rule with calculator and nomogram aids in the triage of patients with suspected GCA and may decrease the need for TABx in select low-score at-risk subjects. However, misclassification remains a concern.
Keywords: diagnosis; giant cell arteritis; nomogram; prediction rule; temporal artery biopsy; validation.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures

Similar articles
-
Neural network and logistic regression diagnostic prediction models for giant cell arteritis: development and validation.Clin Ophthalmol. 2019 Feb 21;13:421-430. doi: 10.2147/OPTH.S193460. eCollection 2019. Clin Ophthalmol. 2019. PMID: 30863010 Free PMC article.
-
Lower ocular pulse amplitude with dynamic contour tonometry is associated with biopsy-proven giant cell arteritis.Can J Ophthalmol. 2018 Jun;53(3):215-221. doi: 10.1016/j.jcjo.2017.10.027. Epub 2017 Dec 26. Can J Ophthalmol. 2018. PMID: 29784156
-
Temporal Artery Biopsy in the Workup of Giant Cell Arteritis: Diagnostic Considerations in a Veterans Administration Cohort.J Neuroophthalmol. 2020 Dec;40(4):450-456. doi: 10.1097/WNO.0000000000001040. J Neuroophthalmol. 2020. PMID: 32868573
-
Temporal Artery Biopsy for Diagnosing Giant Cell Arteritis: A Ten-year Review.J Ophthalmic Vis Res. 2020 Apr 6;15(2):201-209. doi: 10.18502/jovr.v15i2.6738. eCollection 2020 Apr-Jun. J Ophthalmic Vis Res. 2020. PMID: 32308955 Free PMC article. Review.
-
Polymyalgia rheumatica and giant cell arteritis in older patients: diagnosis and pharmacological management.Drugs Aging. 2011 Aug 1;28(8):651-66. doi: 10.2165/11592500-000000000-00000. Drugs Aging. 2011. PMID: 21812500 Review.
Cited by
-
Hyperechogenic intimal lesions and wall thickness of the temporal and facial arteries in elderly patients with arterial occlusions of the eye.RMD Open. 2021 Sep;7(3):e001688. doi: 10.1136/rmdopen-2021-001688. RMD Open. 2021. PMID: 34544823 Free PMC article.
-
Recent Advances in Giant Cell Arteritis.Curr Rheumatol Rep. 2018 Apr 2;20(5):25. doi: 10.1007/s11926-018-0737-1. Curr Rheumatol Rep. 2018. PMID: 29611005 Review.
-
Diagnostic Accuracy of Symptoms, Physical Signs, and Laboratory Tests for Giant Cell Arteritis: A Systematic Review and Meta-analysis.JAMA Intern Med. 2020 Oct 1;180(10):1295-1304. doi: 10.1001/jamainternmed.2020.3050. JAMA Intern Med. 2020. PMID: 32804186 Free PMC article.
-
The Use of a Nomogram to Visually Interpret a Logistic Regression Prediction Model for Giant Cell Arteritis.Neuroophthalmology. 2018 Feb 5;42(5):284-286. doi: 10.1080/01658107.2018.1425728. eCollection 2018 Oct. Neuroophthalmology. 2018. PMID: 30258473 Free PMC article.
-
A new era for giant cell arteritis.Eye (Lond). 2020 Jun;34(6):1013-1026. doi: 10.1038/s41433-019-0608-7. Epub 2019 Oct 3. Eye (Lond). 2020. PMID: 31582795 Free PMC article. Review.
References
-
- De Smit E, Palmer AJ, Hewitt AW. Projected worldwide disease burden from giant cell arteritis by 2050. J Rheumatol. 2015;42(1):119–125. - PubMed
-
- Pieri A, Milligan R, Hegde V, Hennessy C. Temporal artery biopsy: are we doing it right? Int J Health Care Qual Assur. 2013;26(6):559–563. - PubMed
-
- Quinn EM, Kearney DE, Kelly J, Keohane C, Redmond HP. Temporal artery biopsy is not required in all cases of suspected giant cell arteritis. Ann Vasc Surg. 2012;26(5):649–654. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
