

Eosinophilic and non-eosinophilic COPD patients with chronic respiratory failure: neutrophil-to-lymphocyte ratio as an exacerbation marker
- PMID: 29200843
- PMCID: PMC5703161
- DOI: 10.2147/COPD.S147261
Eosinophilic and non-eosinophilic COPD patients with chronic respiratory failure: neutrophil-to-lymphocyte ratio as an exacerbation marker
Abstract
Aim: Increased dyspnea, sputum volume, and purulence are subjective symptoms in COPD patients. To diagnose COPD exacerbations with chronic respiratory failure (CRF) and to assess the requirement for antibiotic treatment, physicians require more objective criteria. We aimed to investigate whether neutrophil-to-lymphocyte ratio (NLR) can be used as an infectious exacerbation marker in COPD patients with CRF.
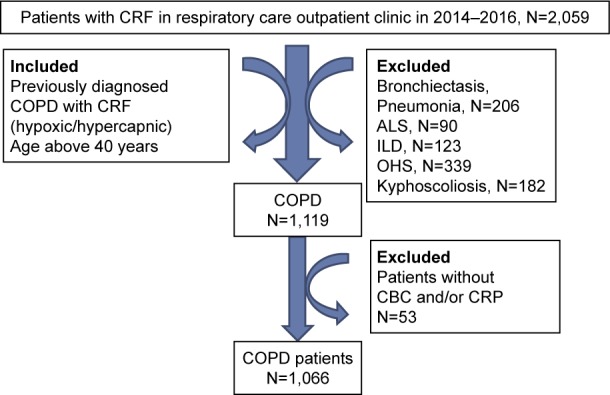
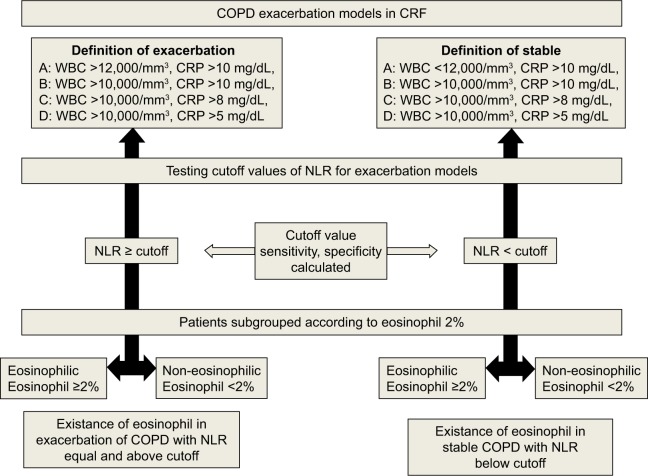
Patients and methods: This retrospective cross-sectional study was performed in the intensive care outpatient clinic of a tertiary training hospital between 2014 and 2015. Patients admitted with CRF due to COPD and who had complete blood count (CBC) results were enrolled. CBC results and C-reactive protein (CRP) levels were obtained from the hospital online database. The "modified exacerbation model (MEM)" was defined as follows: exacerbation A, leukocytes ≥12,000/mm3, CRP >10 mg/dL; exacerbation B, leukocytes ≥10,000/mm3, CRP >10 mg/dL; exacerbation C, leukocytes ≥10,000/mm3, CRP >8 mg/dL; exacerbation D, leukocytes ≥10,000/mm3, CRP >5 mg/dL. The cutoff value of NLR was defined for each model. Patients were split into two groups based on the NLR cutoff value according to the "NLR exacerbation model" and further subgrouped according to peripheral eosinophil percentage (eosinophils ≥2% and <2%) and compared with the MEM.
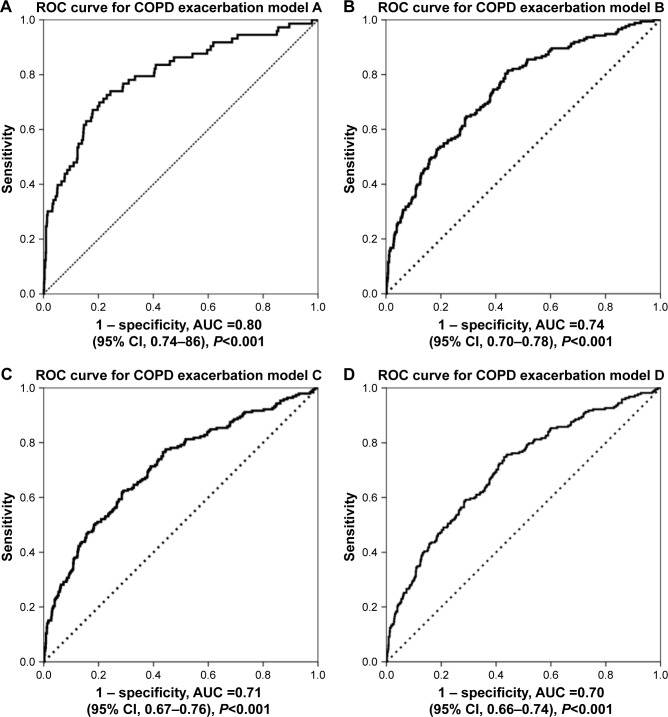
Results: A total of 1,066 COPD patients (430 females, 40.3%), with a mean age of 66±13 years, were included. A NLR cutoff value of 3.54 (NLR ≥3.54, n=366, 34%) showed the highest sensitivity and specificity for model A (78%, 69%), model B (63%, 71%), model C (61%, 72%), and model D (58%, 72%). Peripheral eosinophilia (PE ≥2%) was present in 48 patients (4.5%). The ratio of patients with PE <2% in the NLR ≥3.54 group was significantly higher in the MEM (P<0.001).
Conclusion: The NLR presents an attractive option as an exacerbation marker in COPD patients with CRF due to its simplicity and cost-effectiveness. In COPD patients with CRF, where the NLR is ≥3.54, PE levels are <2%, and subjective symptoms are present, antibiotic treatment should be considered.
Keywords: COPD; chronic respiratory failure; exacerbation; neutrophil-to-lymphocyte ratio; peripheral eosinophilia.
Conflict of interest statement
Disclosure All the authors who contributed to the study design do not have any industry relationships for the past 2 years. The manuscript has been read and approved by all the authors, and each author believes that the manuscript represents honest work. The authors report no conflicts of interest in this work.
Figures
Similar articles
-
The utility of inflammatory markers to predict readmissions and mortality in COPD cases with or without eosinophilia.Int J Chron Obstruct Pulmon Dis. 2015 Nov 11;10:2469-78. doi: 10.2147/COPD.S90330. eCollection 2015. Int J Chron Obstruct Pulmon Dis. 2015. PMID: 26648709 Free PMC article.
-
Does eosinophilic COPD exacerbation have a better patient outcome than non-eosinophilic in the intensive care unit?Int J Chron Obstruct Pulmon Dis. 2015 Sep 8;10:1837-46. doi: 10.2147/COPD.S88058. eCollection 2015. Int J Chron Obstruct Pulmon Dis. 2015. PMID: 26392758 Free PMC article.
-
The neutrophil/lymphocyte ratio is a better addition to C-reactive protein than CD64 index as a marker for infection in COPD.Panminerva Med. 2017 Sep;59(3):203-209. doi: 10.23736/S0031-0808.17.03296-7. Epub 2017 Feb 9. Panminerva Med. 2017. PMID: 28185443
-
Defining the role of neutrophil-to-lymphocyte ratio in COPD: a systematic literature review.Int J Chron Obstruct Pulmon Dis. 2018 Nov 5;13:3651-3662. doi: 10.2147/COPD.S178068. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 30464448 Free PMC article.
-
Prognostic value of platelet and neutrophil to lymphocyte ratio in COPD patients.Expert Rev Respir Med. 2020 Jan;14(1):111-116. doi: 10.1080/17476348.2019.1675517. Epub 2019 Oct 13. Expert Rev Respir Med. 2020. PMID: 31577911 Review.
Cited by
-
Inflammatory Markers in Patients Using Domiciliary Non-invasive Mechanical Ventilation: C Reactive Protein, Procalcitonin, Neutrophil Lymphocyte Ratio.Front Public Health. 2018 Sep 5;6:245. doi: 10.3389/fpubh.2018.00245. eCollection 2018. Front Public Health. 2018. PMID: 30234089 Free PMC article.
-
Prognostic Value of Neutrophil to Lymphocyte Ratio for Predicting 90-Day Poor Outcomes in Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease.Int J Chron Obstruct Pulmon Dis. 2023 Jun 14;18:1219-1230. doi: 10.2147/COPD.S399671. eCollection 2023. Int J Chron Obstruct Pulmon Dis. 2023. PMID: 37337582 Free PMC article.
-
Malnutrition, Airflow Limitation and Severe Emphysema are Risks for Exacerbation of Chronic Obstructive Pulmonary Disease in Japanese Subjects: A Retrospective Single-Center Study.Int J Chron Obstruct Pulmon Dis. 2020 Apr 22;15:857-868. doi: 10.2147/COPD.S238457. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32368031 Free PMC article.
-
Neutrophil-to-lymphocyte ratio can predict outcome in extensive-stage small cell lung cancer.Radiol Oncol. 2020 Sep 22;54(4):437-446. doi: 10.2478/raon-2020-0054. Radiol Oncol. 2020. PMID: 32960780 Free PMC article.
-
The association between neutrophil-lymphocyte ratio and poor outcomes following infant cardiac surgery.BMC Cardiovasc Disord. 2021 Nov 8;21(1):529. doi: 10.1186/s12872-021-02345-3. BMC Cardiovasc Disord. 2021. Retraction in: BMC Cardiovasc Disord. 2024 Oct 26;24(1):596. doi: 10.1186/s12872-024-04285-0. PMID: 34749678 Free PMC article. Retracted.
References
-
- Brightling CE. Biomarkers that predict and guide therapy for exacerbations of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2013;10(suppl):S214–S219. - PubMed
-
- Global Initiative for Chronic Obstructive Lung Disease [home page on Internet] Global Strategy for Diagnosis, Management, and Prevention of COPD (updated 2012) [Accessed August 25, 2016]. Available from: http://www.goldcopd.org.
-
- Anthonisen NR, Manfreda J, Warren CP, et al. Antibiotic therapy in exacerbation of COPD. Ann Intern Med. 1987;106:196–204. - PubMed
-
- Perez-Bogerd S, Fremault A, Decramer M, Janssens W. Criteria for antibiotic therapy in acute exacerbations of COPD. Am J Respir Crit Care Med. 2010;182(9):1207. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
