

Molecular strategies in the management of bronchopulmonary and thymic neuroendocrine neoplasms
- PMID: 29201449
- PMCID: PMC5690952
- DOI: 10.21037/jtd.2017.03.82
Molecular strategies in the management of bronchopulmonary and thymic neuroendocrine neoplasms
Abstract
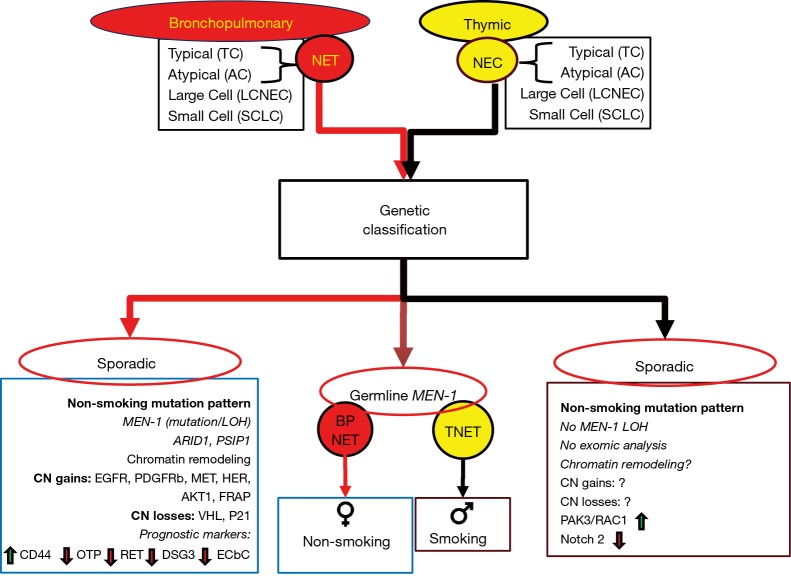
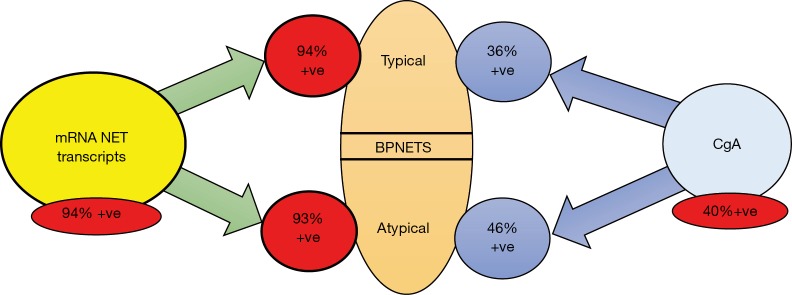
Thoracic NETs [bronchopulmonary NETs (BPNETs) and thymic NETs (TNET)] share a common anatomic primary location, likely a common cell of origin, the "Kulchitsky cell" and presumably, a common etiopathogenesis. Although they are similarly grouped into well-differentiated [typical carcinoids (TC) and atypical carcinoids (AC)] and poorly differentiated neoplasms and both express somatostatin receptors, they exhibit a wide variation in clinical behavior. TNETs are more aggressive, are frequently metastatic, and have a lower 5-year survival rate (~50% vs. ~80%) than BPNETs. They are typically symptomatic, most often secreting ACTH (40% of tumors) but both tumor groups share secretion of common biomarkers including chromogranin A and 5-HIAA. Consistently effective and accurate circulating biomarkers are, however, currently unavailable. Surgery is the primary therapeutic tool for both BPNET and TNETs but there remains little consensus about later interventions e.g., targeted therapy, or how these can be monitored. Genetic analyses have identified different topographies (e.g., significant alterations in chromatin and epigenetic remodeling in BPNETs versus frequent chromosomal abnormalities in TNETs) but there is an absence of clinically actionable mutations in both tumor groups. Liquid biopsies, tools that can measure neoplastic signatures in peripheral blood, can potentially be leveraged to detect disease early i.e., recurrence, predict tumors that may respond to specific therapies and serve as real-time monitors for treatment responses. Recent studies have identified that mRNA transcript analysis in blood effectively identifies both BPNET and TNETs. The clinical utility of this gene expression assay includes use as a diagnostic, confirmation of completeness of surgical resection and use as a molecular management tool to monitor efficacy of PRRT and other therapeutic strategies.
Keywords: Biomarker; NETest; bronchopulmonary; carcinoid; neuroendocrine.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
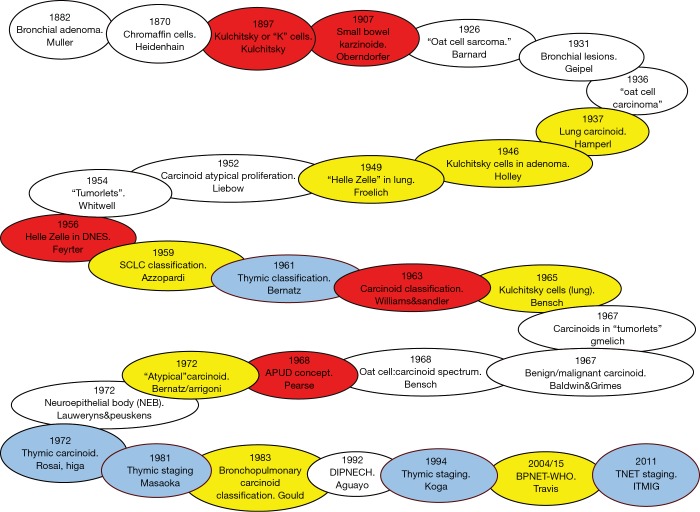
- Geipel P. Concerning Our Knowledge of Benign Bronchial Tumors. Frankfurter Zeitschrift fur Pathologie 1931;42:516.
-
- Arrigoni MG, Woolner LB, Bernatz PE. Atypical carcinoid tumors of the lung. J Thorac Cardiovasc Surg 1972;64:413-21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials