

Neuroendocrine tumors of the thymus
- PMID: 29201451
- PMCID: PMC5690945
- DOI: 10.21037/jtd.2017.10.83
Neuroendocrine tumors of the thymus
Abstract
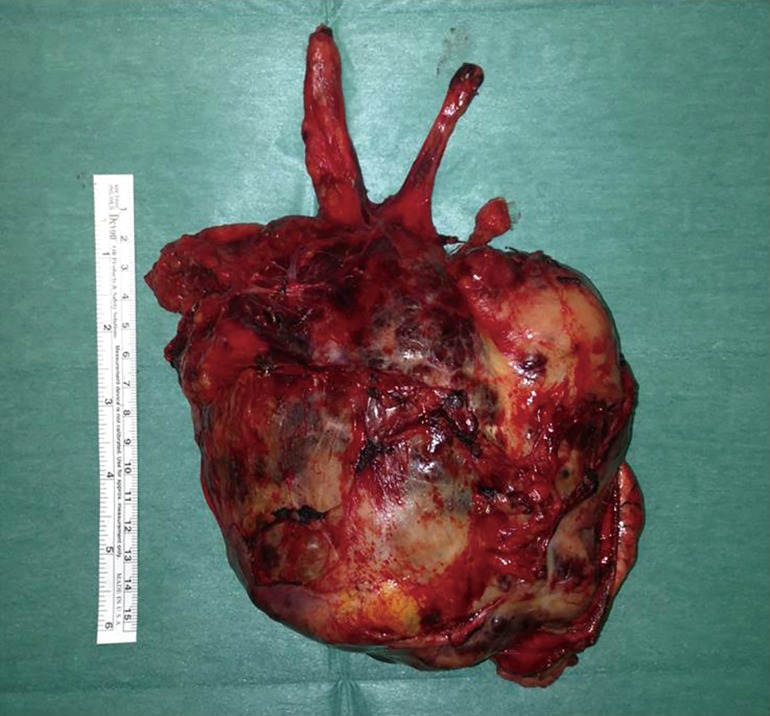
Primary neuroendocrine tumors of the thymus (NETTs) are rare and biologically very aggressive neoplasms, usually located in the anterior mediastinal space. They are more frequently observed in males, in their fourth/fifth decades of life. In 50% of cases, NETTs are associated with endocrinopaties [Cushing's syndrome, acromegaly or Multiple Endocrine Neoplasia-1 (MEN-1) syndrome]. NETTs very often present with invasion of the surrounding mediastinal anatomical structures. Surgery, even in advanced stages, is the mainstay of treatment: a compete resection through a median sternotomy or a combined access (sternotomy + thoracotomy) should be always attempted. Induction chemotherapy (± radiotherapy) is usually administered in advanced neoplasms, with the aim to achieve tumor shinkage, increasing, therefore, the chance to obtain a complete resection. Postoperative radiotherapy (± chemotherapy) is administered in case of invasive lesions, or incomplete resections. NETTs long-term outcome is poor, even in case of completely resected tumors, due to high risk of recurrence or distant metastases development. Prognosis mainly depends on tumor stage, invasivity, completeness of resection, possible association with endocrinopaties and recurrence/distant metastases development.
Keywords: Thymus; diagnosis; neuroendocrine carcinoma; outcome; recurrences; surgery; symptoms.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
-
- Klemm KM, Moran CA. Primary neuroendocrine carcinomas of the thymus. Semin Diagn Pathol 1999;16:32-41. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources