

Biparametric MRI of the prostate
- PMID: 29201499
- PMCID: PMC5687199
- DOI: 10.5152/tud.2017.06978
Biparametric MRI of the prostate
Erratum in
-
Erratum.Turk J Urol. 2018 Jan;44(1):91. doi: 10.5152/tud.2018.0801181. Epub 2017 Jan 1. Turk J Urol. 2018. PMID: 29485140 Free PMC article.
Abstract
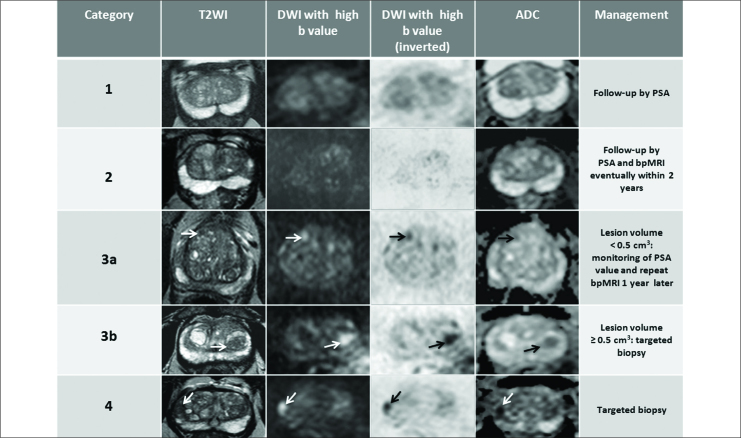
Biparametric Magnetic Resonance Imaging (bpMRI) of the prostate combining both morphologic T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI) is emerging as an alternative to multiparametric MRI (mpMRI) to detect, to localize and to guide prostatic targeted biopsy in patients with suspicious prostate cancer (PCa). BpMRI overcomes some limitations of mpMRI such as the costs, the time required to perform the study, the use of gadolinium-based contrast agents and the lack of a guidance for management of score 3 lesions equivocal for significant PCa. In our experience the optimal and similar clinical results of the bpMRI in comparison to mpMRI are essentially related to the DWI that we consider the dominant sequence for detection suspicious PCa both in transition and in peripheral zone. In clinical practice, the adoption of bpMRI standardized scoring system, indicating the likelihood to diagnose a clinically significant PCa and establishing the management of each suspicious category (from 1 to 4), could represent the rationale to simplify and to improve the current interpretation of mpMRI based on Prostate Imaging and Reporting Archiving Data System version 2 (PI-RADS v2). In this review article we report and describe the current knowledge about bpMRI in the detection of suspicious PCa and a simplified PI-RADS based on bpMRI for management of each suspicious PCa categories to facilitate the communication between radiologists and urologists.
Keywords: Biparametric magnetic resonance imaging; prostate cancer; prostate imaging reporting and data system.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. https://doi.org/10.3322/caac.21166. - DOI - PubMed
-
- Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev. 2010;19:1893–907. https://doi.org/10.1158/1055-9965.EPI-10-0437. - DOI - PubMed
-
- Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P, et al. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2007;18:581–92. https://doi.org/10.1093/annonc/mdl498. - DOI - PubMed
-
- Fine SW, Amin MB, Berney DM, Bjartell A, Egevad L, Epstein JI, et al. A contemporary update on pathology reporting for prostate cancer: biopsy and radical prostatectomy specimens. Eur Urol. 2012;62:20–39. https://doi.org/10.1016/j.eururo.2012.02.055. - DOI - PubMed
-
- Poon PY, McCallum RW, Henkelman MM, Bronskill MJ, Sutcliffe SB, Jewett MA, et al. Magnetic resonance imaging of the prostate. Radiology. 1985;154:143–9. https://doi.org/10.1148/radiology.154.1.2578070. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous