

Adrenocortical carcinoma: Single center experience
- PMID: 29201509
- PMCID: PMC5687209
- DOI: 10.5152/tud.2017.81598
Adrenocortical carcinoma: Single center experience
Abstract
Objective: Adrenocortical carcinoma is an aggressive endocrine malignancy with an annual incidence of 0.5-2 cases per million. The most important factors that determine prognosis are tumor stage at the time of diagnosis and the success of surgery. However, advanced age, large tumor size, hormone secretion, high Ki-67 index (>10%), tumor necrosis and high mitotic activity are other factors associated with poor prognosis. In the present study, we aimed to evaluate the contribution of the patient and treatment- related factors to the prognosis in adrenocortical carcinoma.
Material and methods: We included 15 adrenocortical carcinoma patients who were followed in our center between 2005 and 2015. The effects of age, gender, tumor size, type of operation, postoperative resection status and adjuvant treatment on disease-free survival and overall survival were analyzed.
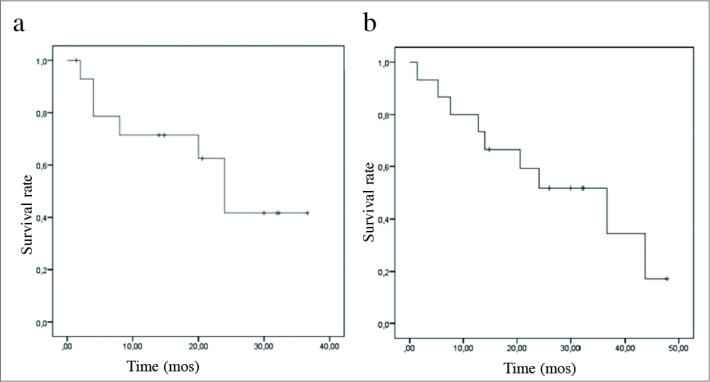
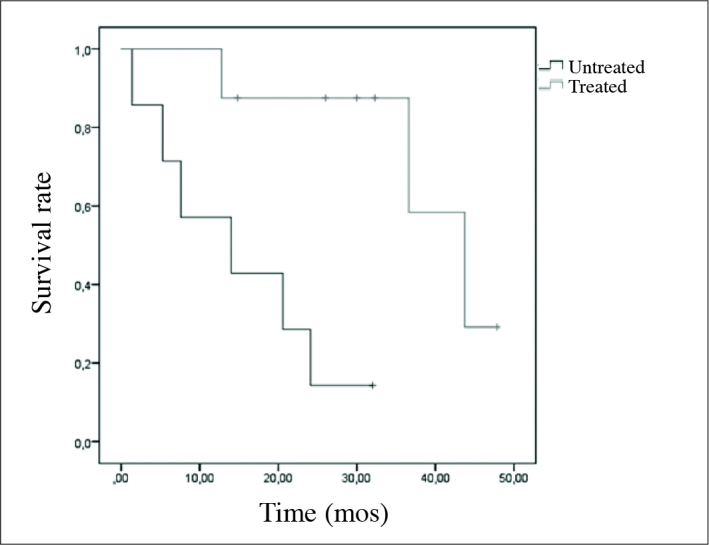
Results: Disease-free survival was 23.32±3.69 months and overall survival was 36.60±10.78 months. Gender, tumor size, tumor stage, type of operation, hormonal activity, presence of necrosis, recurrence and development of metastasis were not found to be associated with disease-free survival and overall survival (p>0.05). Postoperatively applied adjuvant treatments including mitotane, chemotherapy and radiotherapy did not significantly affect disease-free survival in our study, but statistically significant increase in overall survival was observed in patients getting adjuvant treatments (p=0.006).
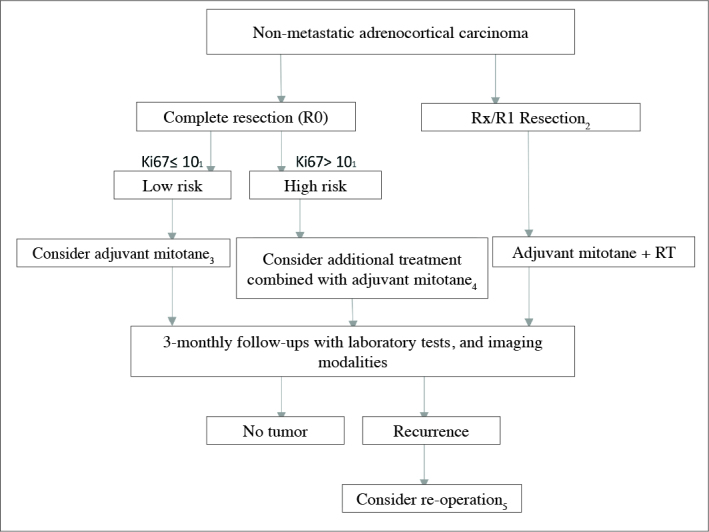
Conclusion: Adrenocortical carcinoma has poor prognosis and short overall survival, and in its clinical course, recurrence and development of metastasis can be commonly observed even after complete resection of the tumor. Therefore, the patients should be evaluated carefully while determining the surgical procedure during the preoperative period, and the operation and post-operative follow-up should be performed in experienced centers. However, due to the positive effects of adjuvant treatments on survival, all patients should be evaluated postoperatively for the necessity of adjuvant treatments, especially mitotane.
Keywords: Adrenocortical carcinoma; chemotherapy; mitotane; surgery.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures
References
-
- Michalkiewicz E, Sandrini R, Figueiredo B, Miranda EC, Caran E, Oliveira-Filho AG, et al. Clinical and outcome characteristics of children with adrenocortical tumors: a report from the International Pediatric Adrenocortical Tumor Registry. J Clin Oncol. 2004;22:838–45. https://doi.org/10.1200/JCO.2004.08.085. - DOI - PubMed
-
- Berruti A, Baudin E, Gelderblom H, Haak HR, Porpiglia F, Fassnacht M, et al. Adrenal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23(Suppl 7):vii131–8. https://doi.org/10.1093/annonc/mds231. - DOI - PubMed
-
- Allolio B, Fassnacht M. Clinical review: Adrenocortical carcinoma: clinical update. J Clin Endocrinol Metab. 2006;91:2027–37. https://doi.org/10.1210/jc.2005-2639. - DOI - PubMed
-
- Elsayes KM, Emad-Eldin S, Morani AC, Jensen CT. Practical approach to adrenal imaging. Radiol Clin North Am. 2017;55:279–301. https://doi.org/10.1016/j.rcl.2016.10.005. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources