

Urinary matrix metalloproteinase 9 and tissue inhibitor of metalloproteinase 1 biomarkers for predicting renal scar in children with urinary tract infection
- PMID: 29201521
- PMCID: PMC5687221
- DOI: 10.5152/tud.2017.06337
Urinary matrix metalloproteinase 9 and tissue inhibitor of metalloproteinase 1 biomarkers for predicting renal scar in children with urinary tract infection
Abstract
Objective: Urinary tract infection occurs in 1.8-6.6% of children under 6 years old. The aim of this study was to assess the urinary concentrations of matrix metalloproteinase 9 (MMP9) and tissue inhibitor of metalloproteinase 1 (TIMP1), in children with acute pyelonephritis (APN) and the potential to develop renal scarring.
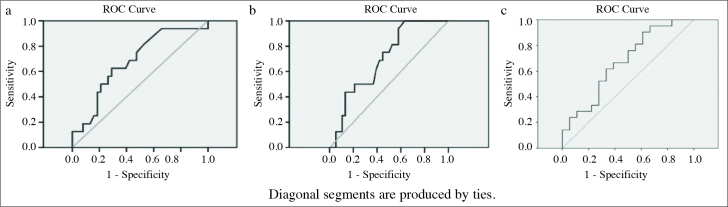
Material and methods: Children who had experienced an episode of APN were divided into 2 groups. Group 1 included children with APN who exhibited scarring and group 2 included children with APN who had a normal 99mTechnetium dimercaptosuccinic acid scan. Urinary levels of MMP9 and TIMP1 were measured in the acute phase of infection. A receiver operating characteristic curve was generated to allow calculation of cut-off values.
Results: Sixty-one children were enrolled across the 2 groups: group 1 contained 16 patients (all female); group 2, 38 children (36 female and 2 male). Urinary levels of MMP9 and TIMP1 were significantly higher in group 1 than in group 2 (p=0.037 and 0.022 respectively). For comparison of groups 1 and 2, the cut-off values were measured as 75.5 ng/mL (sensitivity 62.5%, specificity 71.1%, positive predictive value, PPV, 48%, negative predictive value, NPV, 82%), 16.1 ng/mL (sensitivity 75%, specificity 55.3%, PPV 41%, NPV 84%), and 1310.7 ng/mL (sensitivity 75% specificity 60.5%, PPV 44%, NPV 85%) for MMP9, TIMP1, and MMP9×TIMP1 levels, respectively.
Conclusion: Evaluation of urinary MMP9 and TIMP1 levels may help to identify children with APN who are at risk of developing renal scarring.
Keywords: Children; matrix metalloproteinase; pyelonephritis; tissue inhibitor of metalloproteinase 1; urinary tract infection; vesico-ureteral reflux.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures
Similar articles
-
The role of urinary TIMP1 and MMP9 levels in predicting vesicoureteral reflux in neonates with antenatal hydronephrosis.Pediatr Nephrol. 2014 May;29(5):871-8. doi: 10.1007/s00467-013-2693-3. Epub 2014 Jan 4. Pediatr Nephrol. 2014. PMID: 24389602
-
Urinary neutrophil gelatinase-associated lipocalin (NGAL) might be an independent marker for anticipating scar formation in children with acute pyelonephritis.J Renal Inj Prev. 2015 Jun 1;4(2):39-44. doi: 10.12861/jrip.2015.09. eCollection 2015. J Renal Inj Prev. 2015. PMID: 26060836 Free PMC article.
-
Matrix metalloproteinase 9 and tissue inhibitor of metalloproteinase 1 in vesicoureteral reflux.Pediatr Nephrol. 2012 Mar;27(3):435-41. doi: 10.1007/s00467-011-2026-3. Epub 2011 Oct 5. Pediatr Nephrol. 2012. PMID: 21969093
-
Dimercaptosuccinic acid scan challenges in childhood urinary tract infection, vesicoureteral reflux and renal scarring investigation and management.Minerva Urol Nefrol. 2017 Apr;69(2):144-152. doi: 10.23736/S0393-2249.16.02509-1. Epub 2016 Jun 29. Minerva Urol Nefrol. 2017. PMID: 27355216 Review.
-
Update on dimercaptosuccinic acid renal scanning in children with urinary tract infection.Pediatr Nephrol. 1995 Apr;9(2):221-6; discussion 227. doi: 10.1007/BF00860755. Pediatr Nephrol. 1995. PMID: 7794724 Review.
Cited by
-
Urinary Tract Infections Detection with Molecular Biomarkers.Biomolecules. 2024 Nov 30;14(12):1540. doi: 10.3390/biom14121540. Biomolecules. 2024. PMID: 39766247 Free PMC article. Review.
-
Selected Metal Matrix Metalloproteinases and Tissue Inhibitors of Metalloproteinases as Potential Biomarkers for Tubulointerstitial Fibrosis in Children with Unilateral Hydronephrosis.Dis Markers. 2020 Jun 29;2020:9520309. doi: 10.1155/2020/9520309. eCollection 2020. Dis Markers. 2020. PMID: 32670438 Free PMC article.
References
-
- Saadeh SA, Mattoo TK. Managing urinary tract infections. Pediatr Nephrol. 2011;26:1967–76. https://doi.org/10.1007/s00467-011-1801-5. - DOI - PMC - PubMed
-
- Hoberman A, Charron M, Hickey RW, Baskin M, Kearney DH, Wald ER. Imaging studies after a first febrile urinary tract infection in young children. N Engl J Med. 2003;348:195–202. https://doi.org/10.1056/NEJMoa021698. - DOI - PubMed
-
- Peters CA, Skoog SJ, Arant BS, Jr, Copp HL, Elder JS, Hudson RG, et al. Summary of the AUA guideline on management of primary vesicoureteral reflux in children. J Urol. 2010;184:1134–44. https://doi.org/10.1016/j.juro.2010.05.065. - DOI - PubMed
-
- Jahnukainen T, Chen M, Celsi G. Mechanisms of renal damage owing to infection. Pediatr Nephrol. 2005;20:1043–53. https://doi.org/10.1007/s00467-005-1898-5. - DOI - PubMed
-
- Abedi SM, Mohammadjafari H, Hosseinimehr SJ, Mardanshahi A, Shahhosseini R. Imaging of renal cortex in nuclear medicine. Journal of Clinical Excellence. 2014;2:50–69.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous