

Clinical presentation, epidemiology, neurophysiological findings, treatment and outcome of nonconvulsive status epilepticus: a 3-year prospective, hospital-based study
- PMID: 29201532
- PMCID: PMC5700530
- DOI: 10.1080/21556660.2017.1396992
Clinical presentation, epidemiology, neurophysiological findings, treatment and outcome of nonconvulsive status epilepticus: a 3-year prospective, hospital-based study
Abstract
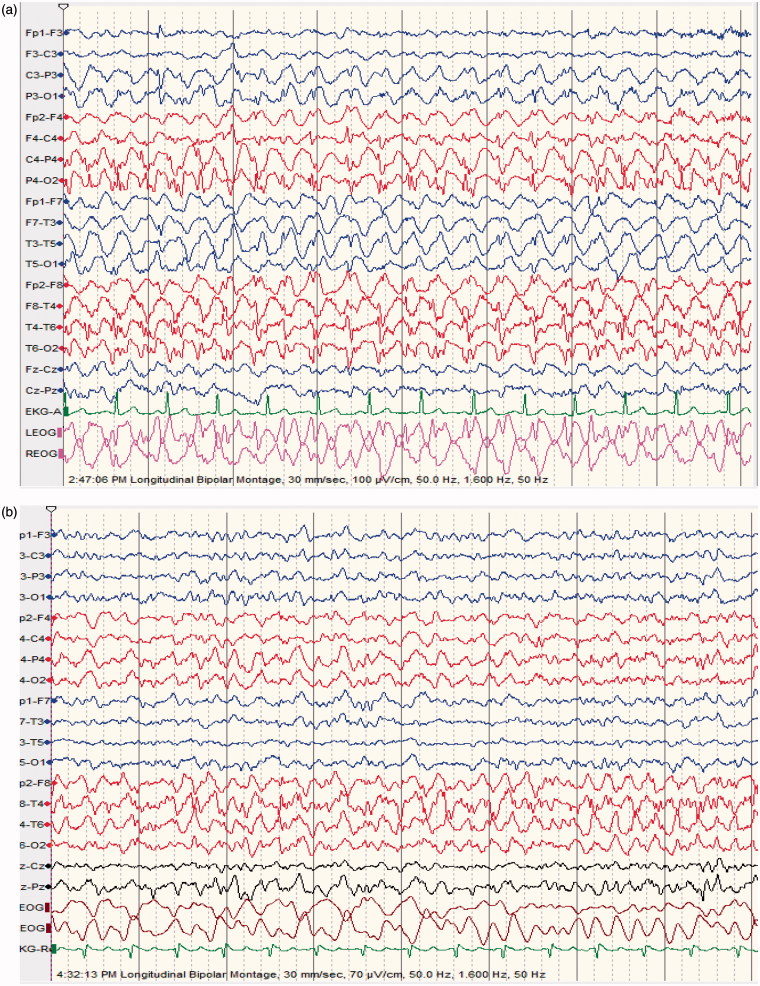
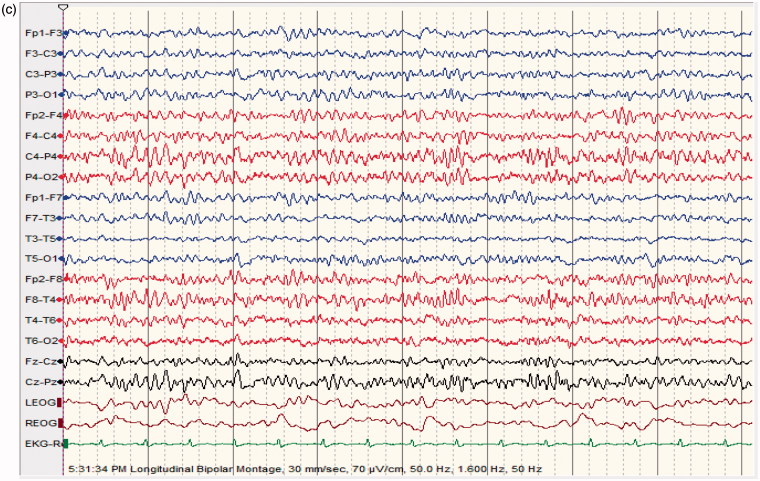
Objective: This study reports the prevalence of Nonconvulsive Status Epilepticus (NCSE) in patients with altered mental status (AMS), and describes the clinical presentation, etiology, neurophysiological findings, neuroimaging, treatment, and outcome of NCSE in Qatar. Recording duration of continuous EEG monitoring was also discussed. Methods: This was a 3-year, prospective, hospital-based study involving patients with AMS and continuous EEG monitoring admitted to the Emergency and ICUs of Hamad Hospital, Qatar. Patients with confirmed diagnosis of NCSE were compared to the patients who did not show EEG and clinical features compatible with NCSE. Descriptive statistics in terms of mean with standard deviation, as well as frequency and percentages for categorical variables, were calculated; Student's t test as well as Chi-square tests or Fisher's exact tests were applied. Logistic regressions NSCE was performed using significance level 0.05 for independent variables at univariate analysis. Results: Number of patients with AMS and continuous EEG monitoring was 250. Number of patients with EEG compatible with NCSE: 65 (age range, 12-79 ys; m, 37; f, 28). Number of controls (defined as patients with EEG not compatible with NCSE): 185 (age range, 12-80 ys; m, 101; f, 84). Rate of occurrence of NCSE in patients with AMS: 26%. NCSE group was younger than controls (p < .001). Twenty patients with NCSE (31%) and 35 patients in the control group (19%) died. Death was more frequent in comatose NCSE compared to controls (p < .0007). NCSE proper and comatose NCSE had longer hospital stays than controls (p < .02 and p < .03, respectively). Complete recovery occurred in 26 NCSE patients (40%) and in 98 controls (53%) (p < .08). Twenty-one patients (31%) presented with refractory NCSE: 12 patients survived, 9 died. Conclusion: This was the first prospective study reporting a high number of NCSE in Qatar, a small country in the MENA region. This prevalence (26%) was in the middle range. NCSE patients did not perform better than controls, outcome being worse with comatose NCSE. NCSE is an emergent condition warranting expedited diagnosis and management. Three days of continuous EEG monitoring were able to diagnose most cases of NCSE.
Keywords: NCSE; cEEG monitoring; epidemiology; outcome; treatment.
Figures


References
-
- Kinney MO, Craig JJ, Kaplan PW.. Hidden in plain sight: non-convulsive status epilepticus-recognition and management. Acta Neurol Scand. 2017;136(4):280–292. - PubMed
-
- Kaplan PW. Nonconvulsive status epilepticus in the emergency room. Epilepsia. 1996;37(7):643–650. - PubMed
-
- Rüegg S. Non-convulsive status epilepticus in adults: an overview. Schweiz Arch Neurol Psychiatr. 2008;159:53–83.
-
- Knake S, Rosenow F, Vescovi M, et al. Incidence of status epilepticus in adults in Germany: a prospective, population-based study. Epilepsia. 2001;42:714–718. - PubMed
-
- Maganti R, Gerber P, Drees C, et al. Nonconvulsive status epilepticus. Epilepsy Behav. 2008;12:572–586 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials