

Brain lesions affecting gait recovery in stroke patients
- PMID: 29201557
- PMCID: PMC5698874
- DOI: 10.1002/brb3.868
Brain lesions affecting gait recovery in stroke patients
Abstract
Objectives: Gait recovery is an important goal in stroke patients. Several studies have sought to uncover relationships between specific brain lesions and the recovery of gait, but the effects of specific brain lesions on gait remain unclear. Thus, we investigated the effects of stroke lesions on gait recovery in stroke patients.
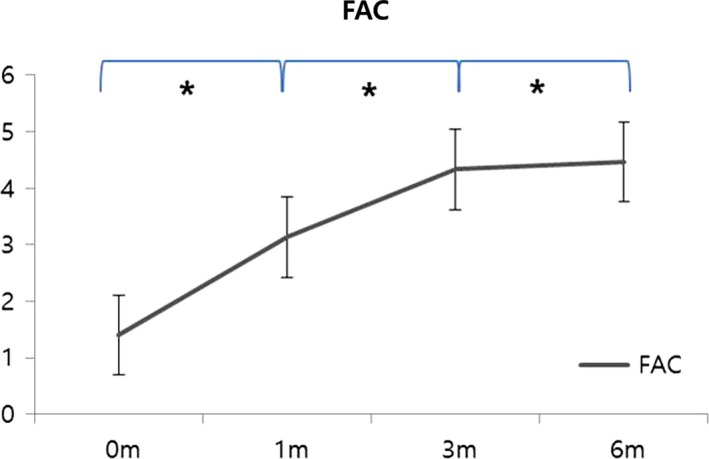
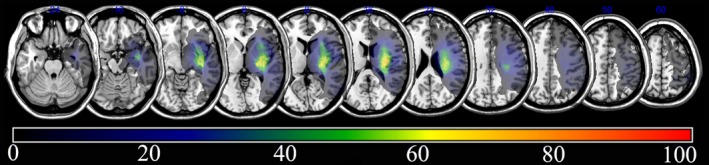
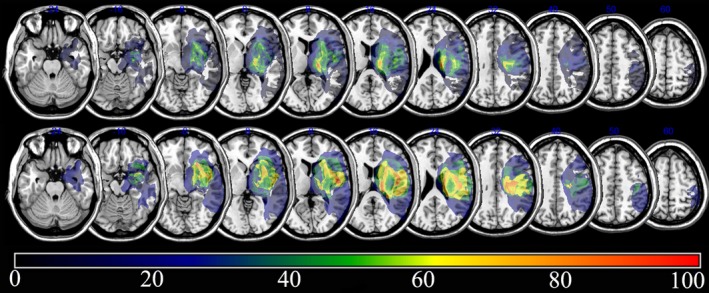
Materials and methods: In total, 30 subjects with stroke were assessed in a retrograde longitudinal observational study. To assess gait function, the functional ambulation category (FAC) was tested four times: initially (within 2 weeks) and 1, 3, and 6 months after the onset of the stroke. Brain lesions were analyzed via overlap, subtraction, and voxel-based lesion symptom mapping (VLSM).
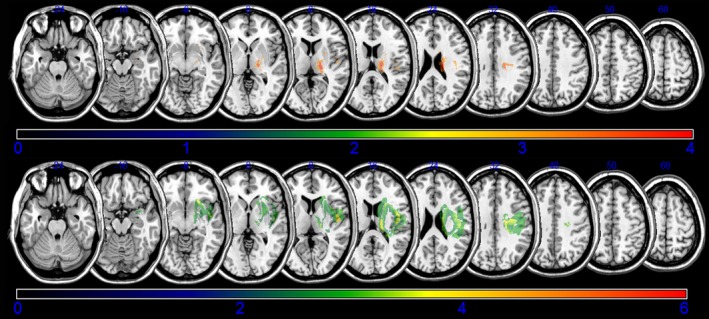
Results: Ambulation with FAC improved significantly with time. Subtraction analysis showed that involvement of the corona radiata, internal capsule, globus pallidus, and putamen were associated with poor recovery of gait throughout 6 months after onset. The caudate nucleus did influence poor recovery of gait at 6 months after onset. VLSM revealed that corona radiata, internal capsule, globus pallidus, putamen and cingulum were related with poor recovery of gait at 3 months after onset. Corona radiata, internal capsule, globus pallidus, putamen, primary motor cortex, and caudate nucleus were related with poor recovery of gait at 6 months after onset.
Conclusion: Results identified several important brain lesions for gait recovery in patients with stroke. These results may be useful for planning rehabilitation strategies for gait and understanding the prognosis of gait in stroke patients.
Keywords: brain lesion; gait; lesion symptom mapping; recovery; stroke.
Figures
References
-
- Ada, L. , Dean, C. M. , Vargas, J. , & Ennis, S. (2010). Mechanically assisted walking with body weight support results in more independent walking than assisted overground walking in non‐ambulatory patients early after stroke: A systematic review. Journal of Physiotherapy, 56, 153–161. - PubMed
-
- Alexander, L. D. , Black, S. E. , Patterson, K. K. , Gao, F. , Danells, C. J. , & McIlroy, W. E. (2009). Association between gait asymmetry and brain lesion location in stroke patients. Stroke, 40, 537–544. https://doi.org/510.1161/STROKEAHA.1108.527374 - PubMed
-
- Brett, M. , Leff, A. P. , Rorden, C. , & Ashburner, J. (2001). Spatial normalization of brain images with focal lesions using cost function masking. NeuroImage, 14, 486–500. - PubMed
-
- Chen, C. L. , Tang, F. T. , Chen, H. C. , Chung, C. Y. , & Wong, M. K. (2000). Brain lesion size and location: Effects on motor recovery and functional outcome in stroke patients. Archives of Physical Medicine and Rehabilitation, 81, 447–452. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
