

Moving from medical to health systems classifications of deaths: extending verbal autopsy to collect information on the circumstances of mortality
- PMID: 29202052
- PMCID: PMC5675065
- DOI: 10.1186/s41256-016-0002-y
Moving from medical to health systems classifications of deaths: extending verbal autopsy to collect information on the circumstances of mortality
Erratum in
-
Erratum to: Moving from medical to health systems classifications of deaths: extending verbal autopsy to collect information on the circumstances of mortality.Glob Health Res Policy. 2016 Jul 19;1:7. doi: 10.1186/s41256-016-0008-5. eCollection 2016. Glob Health Res Policy. 2016. PMID: 29205231 Free PMC article.
Abstract
Background: Verbal autopsy (VA) is a health surveillance technique used in low and middle-income countries to establish medical causes of death (CODs) for people who die outside hospitals and/or without registration. By virtue of the deaths it investigates, VA is also an opportunity to examine social exclusion from access to health systems. The aims were to develop a system to collect and interpret information on social and health systems determinants of deaths investigated in VA.
Methods: A short set of questions on care pathways, circumstances and events at and around the time of death were developed and integrated into the WHO 2012 short form VA (SF-VA). Data were subsequently analysed from two census rounds in the Agincourt Health and Socio-Demographic Surveillance Site (HDSS), South Africa in 2012 and 2013 where the SF-VA had been applied. InterVA and descriptive analysis were used to calculate cause-specific mortality fractions (CSMFs), and to examine responses to the new indicators and whether and how they varied by medical CODs and age/sex sub-groups.
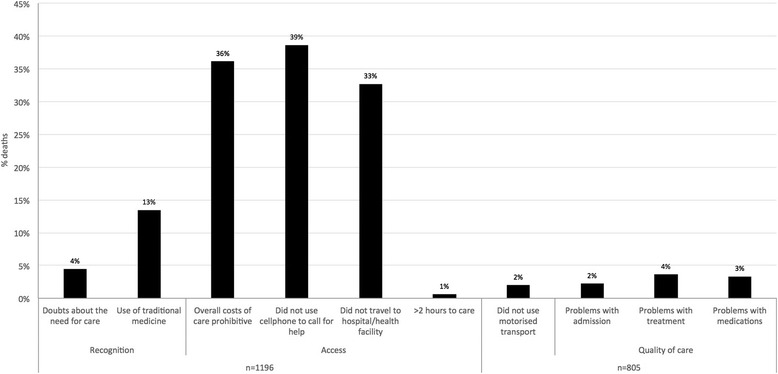
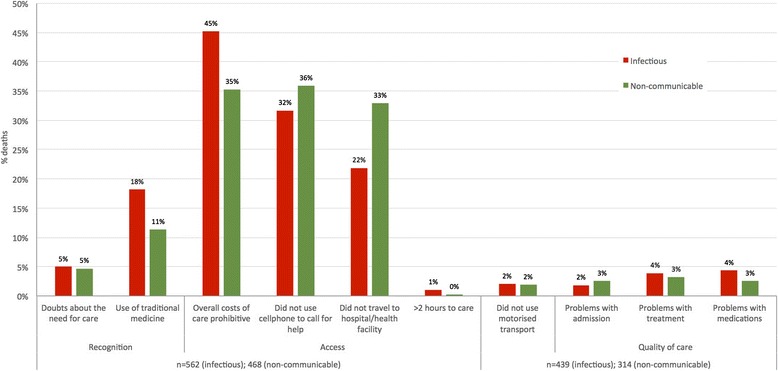
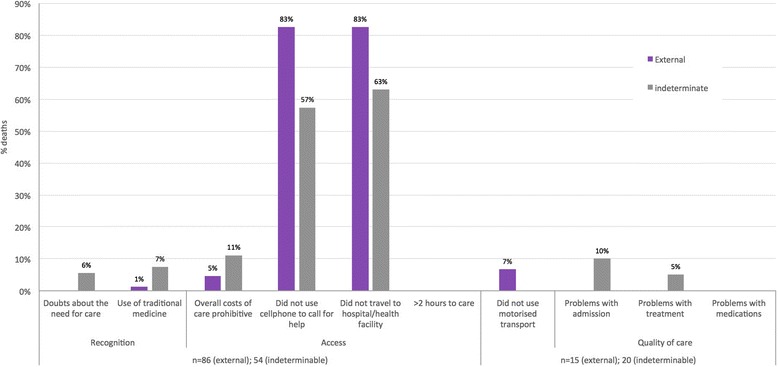
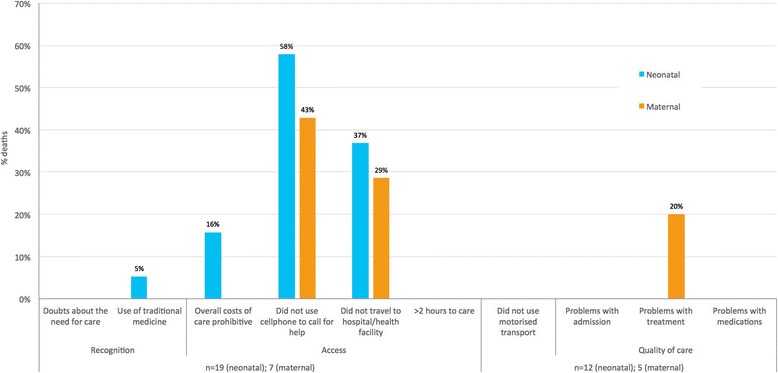
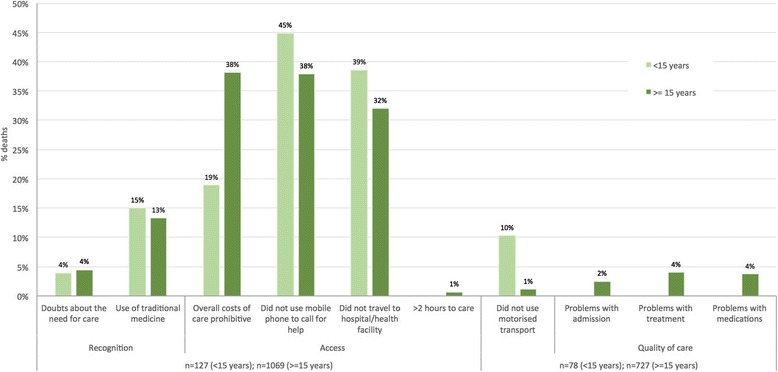
Results: One thousand two hundred forty-nine deaths were recorded in the Agincourt HDSS censuses in 2012-13 of which 1,196 (96 %) had complete VA data. Infectious and non-communicable conditions accounted for the majority of deaths (47 % and 39 % respectively) with smaller proportions attributed to external, neonatal and maternal causes (5 %, 2 % and 1 % respectively). 5 % of deaths were of indeterminable cause. The new indicators revealed multiple problems with access to care at the time of death: 39 % of deaths did not call for help, 36 % found care unaffordable overall, and 33 % did not go to a facility. These problems were reported consistently across age and sex sub-groups. Acute conditions and younger age groups had fewer problems with overall costs but more with not calling for help or going to a facility. An illustrative health systems interpretation suggests extending and promoting existing provisions for transport and financial access in this setting.
Conclusions: Supplementing VA with questions on the circumstances of mortality provides complementary information to CSMFs relevant for health planning. Further contextualisation of the method and results are underway with health systems stakeholders to develop the interpretation sequence as part of a health policy and systems research approach.
Keywords: Civil registration and vital statistics; Health surveillance; Health systems; Social determinants; South Africa; Verbal autopsy.
Figures

Similar articles
-
Enhancing the value of mortality data for health systems: adding Circumstances Of Mortality CATegories (COMCATs) to deaths investigated by verbal autopsy.Glob Health Action. 2019;12(1):1680068. doi: 10.1080/16549716.2019.1680068. Glob Health Action. 2019. PMID: 31648624 Free PMC article.
-
Refining circumstances of mortality categories (COMCAT): a verbal autopsy model connecting circumstances of deaths with outcomes for public health decision-making.Glob Health Action. 2021 Oct 26;14(sup1):2000091. doi: 10.1080/16549716.2021.2000091. Glob Health Action. 2021. PMID: 35377291 Free PMC article.
-
Synthesizing a pragmatic and systemized measure of universal health coverage: verifying the circumstances of mortality CATegories of death investigated by verbal autopsy.Front Public Health. 2025 Apr 3;13:1422248. doi: 10.3389/fpubh.2025.1422248. eCollection 2025. Front Public Health. 2025. PMID: 40247880 Free PMC article.
-
Estimating causes of death where there is no medical certification: evolution and state of the art of verbal autopsy.Glob Health Action. 2021 Oct 26;14(sup1):1982486. doi: 10.1080/16549716.2021.1982486. Glob Health Action. 2021. PMID: 35377290 Free PMC article. Review.
-
Levels and Causes of Maternal Mortality and Morbidity.In: Black RE, Laxminarayan R, Temmerman M, Walker N, editors. Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Apr 5. Chapter 3. In: Black RE, Laxminarayan R, Temmerman M, Walker N, editors. Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2016 Apr 5. Chapter 3. PMID: 27227230 Free Books & Documents. Review.
Cited by
-
Mortality trends and access to care for cardiovascular diseases in Agincourt, rural South Africa: a mixed-methods analysis of verbal autopsy data.BMJ Open. 2021 Jun 25;11(6):e048592. doi: 10.1136/bmjopen-2020-048592. BMJ Open. 2021. PMID: 34172550 Free PMC article.
-
Introducing visual participatory methods to develop local knowledge on HIV in rural South Africa.BMJ Glob Health. 2017 Sep 28;2(3):e000231. doi: 10.1136/bmjgh-2016-000231. eCollection 2017. BMJ Glob Health. 2017. PMID: 29071128 Free PMC article.
-
Care pathways during a child's final illness in rural South Africa: Findings from a social autopsy study.PLoS One. 2019 Oct 22;14(10):e0224284. doi: 10.1371/journal.pone.0224284. eCollection 2019. PLoS One. 2019. PMID: 31639177 Free PMC article.
-
The trend and pattern of adult mortality in South-Central Ethiopia: analysis using the 2008-2019 data from Butajira Health and Demographic Surveillance System.Glob Health Action. 2022 Dec 31;15(1):2118180. doi: 10.1080/16549716.2022.2118180. Glob Health Action. 2022. PMID: 36178408 Free PMC article.
-
Place of death, care-seeking and care pathway progression in the final illnesses of children under five years of age in sub-Saharan Africa: a systematic review.J Glob Health. 2019 Dec;9(2):020422. doi: 10.7189/jogh.09.020422. J Glob Health. 2019. PMID: 31673338 Free PMC article.
References
-
- Agincourt Population and Health Unit . Census results 2011. Johannesburg: University of the Witwatersrand, South Africa; 2011.
-
- Bird J, Byass P, Kahn K, Fottrell E. (2013). A matter of life and death: Practical and ethical constraints in the development of a mobile verbal autopsy tool. Conference: Proceedings of the SIGCHI 2013 Proceedings of the SIGCHI Conference on Human Factors in Computing Systems Pages 1489–1498 DOI:10.1145/2470654.2466198. Available at:http://dl.acm.org/citation.cfm?id=2466198
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
