

Community-based management versus traditional hospitalization in treatment of drug-resistant tuberculosis: a systematic review and meta-analysis
- PMID: 29202059
- PMCID: PMC5693550
- DOI: 10.1186/s41256-016-0010-y
Community-based management versus traditional hospitalization in treatment of drug-resistant tuberculosis: a systematic review and meta-analysis
Abstract
Background: Multidrug drug resistant Tuberculosis (MDR-TB) and extensively drug resistant Tuberculosis (XDR-TB) have emerged as significant public health threats worldwide. This systematic review and meta-analysis aimed to investigate the effects of community-based treatment to traditional hospitalization in improving treatment success rates among MDR-TB and XDR-TB patients in the 27 MDR-TB High burden countries (HBC).
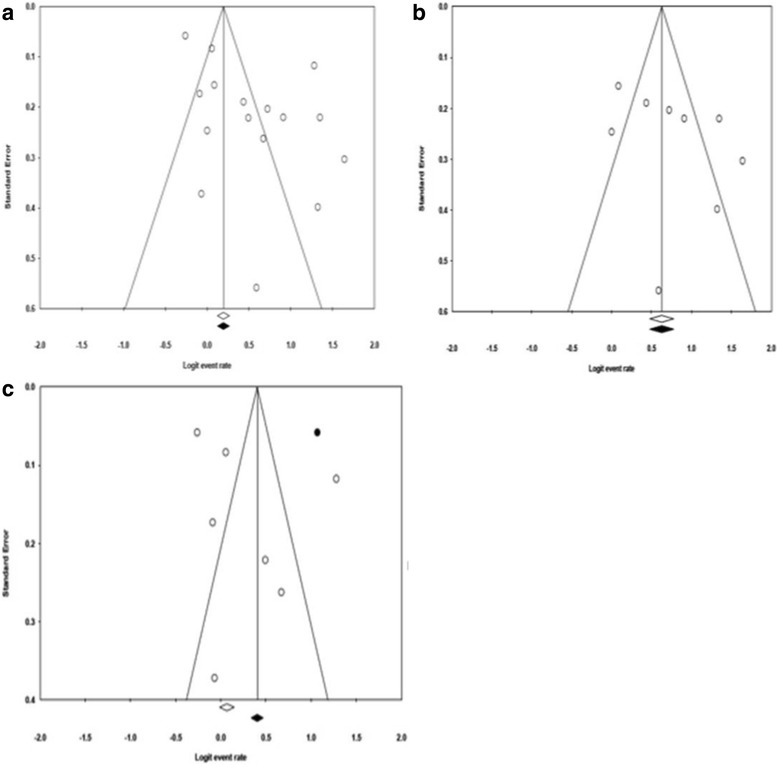
Methods: We searched PubMed, Cochrane, Lancet, Web of Science, International Journal of Tuberculosis and Lung Disease, and Centre for Reviews and Dissemination (CRD) for studies on community-based treatment and traditional hospitalization and MDR-TB and XDR-TB from the 27 MDR-TB HBC. Data on treatment success and failure rates were extracted from retrospective and prospective cohort studies, and a case control study. Sensitivity analysis, subgroup analyses, and meta-regression analysis were used to explore bias and potential sources of heterogeneity.
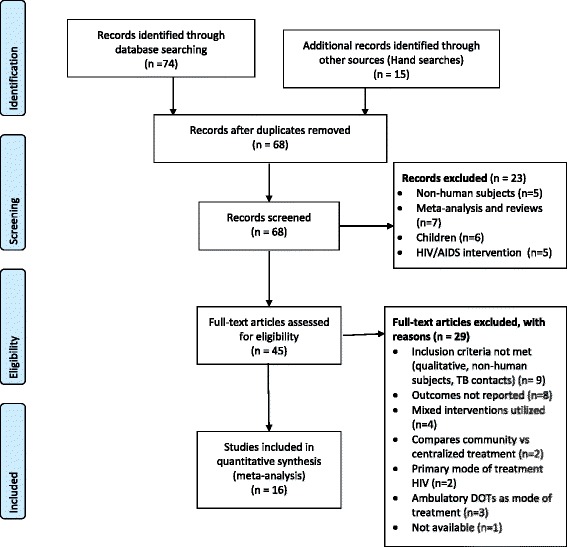
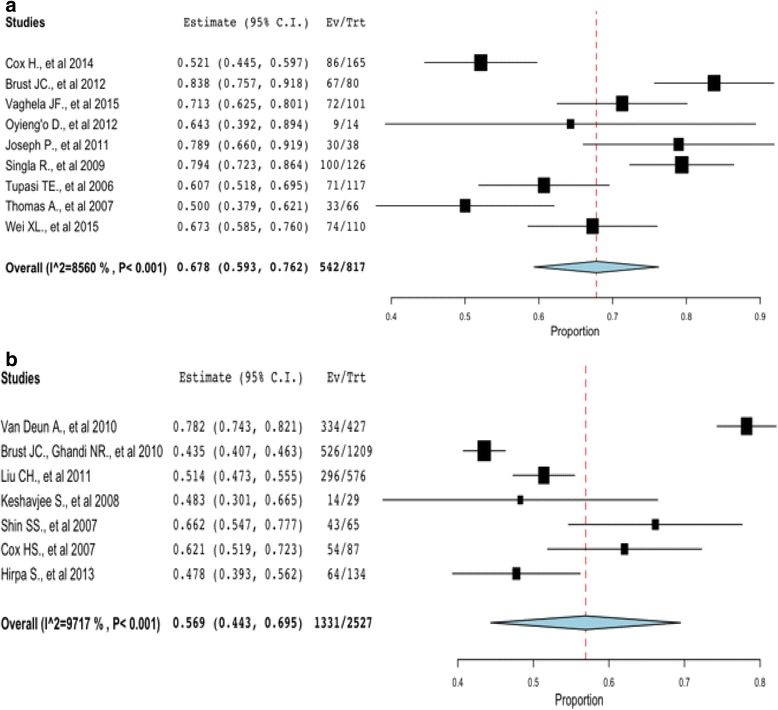
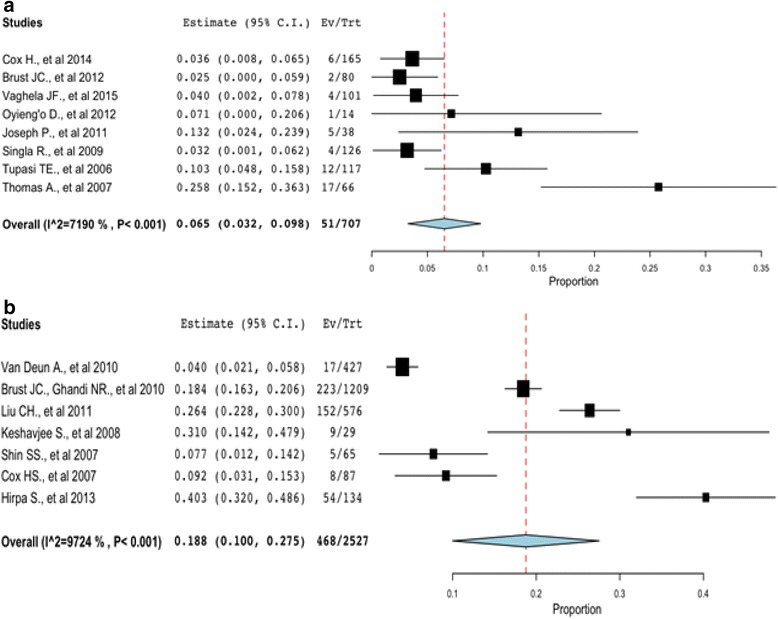
Results: The final sample included 16 studies involving 3344 patients from nine countries; Bangladesh, China, Ethiopia, Kenya, India, South Africa, Philippines, Russia, and Uzbekistan. Based on a random-effects model, we observed a higher treatment success rate in community-based treatment (Point estimate = 0.68, 95 % CI: 0.59 to 0.76, p < 0.01) compared to traditional hospitalization (Point estimate = 0.57, 95 % CI: 0.44 to 0.69, p < 0.01). A lower treatment failure rate was observed in community-based treatment 7 % (Point estimate = 0.07, 95 % CI: 0.03 to 0.10; p < 0.01) compared to traditional hospitalization (Point estimate = 0.188, 95 % CI: 0.10 to 0.28; p < 0.01). In the subgroup analysis, studies without HIV co-infected patients, directly observed therapy short course-plus (DOTS-Plus) implemented throughout therapy, treatment duration > 18 months, and regimen with drugs >5 reported higher treatment success rate. In the meta-regression model, age of patients, adverse events, treatment duration, and lost to follow up explains some of the heterogeneity of treatment effects between studies.
Conclusion: Community-based management improved treatment outcomes. A mix of interventions with DOTS-Plus throughout therapy and treatment duration > 18 months as well as strategies in place for lost to follow up and adverse events should be considered in MDR-TB and XDR-TB interventions, as they influenced positively, treatment success.
Keywords: Community-based treatment; Extensively drug resistant tuberculosis; Hospitalization; MDR-TB high burden countries; Multidrug resistant tuberculosis.
Figures
Similar articles
-
Prevalence of long-term physical sequelae among patients treated with multi-drug and extensively drug-resistant tuberculosis: a systematic review and meta-analysis.EClinicalMedicine. 2023 Mar 10;57:101900. doi: 10.1016/j.eclinm.2023.101900. eCollection 2023 Mar. EClinicalMedicine. 2023. PMID: 36942158 Free PMC article.
-
Predictors of multidrug- and extensively drug-resistant tuberculosis in a high HIV prevalence community.PLoS One. 2010 Dec 29;5(12):e15735. doi: 10.1371/journal.pone.0015735. PLoS One. 2010. PMID: 21209951 Free PMC article.
-
Multidrug and extensively drug-resistant TB (M/XDR-TB): problems and solutions.Indian J Tuberc. 2010 Oct;57(4):180-91. Indian J Tuberc. 2010. PMID: 21141336 Review.
-
Decline in rates of acquired multidrug-resistant tuberculosis after implementation of the directly observed therapy, short course (DOTS) and DOTS-Plus programmes in Taiwan.J Antimicrob Chemother. 2013 Aug;68(8):1910-6. doi: 10.1093/jac/dkt103. Epub 2013 Apr 10. J Antimicrob Chemother. 2013. PMID: 23580558
-
Clinical management of adults and children with multidrug-resistant and extensively drug-resistant tuberculosis.Clin Microbiol Infect. 2017 Mar;23(3):131-140. doi: 10.1016/j.cmi.2016.10.008. Epub 2016 Oct 15. Clin Microbiol Infect. 2017. PMID: 27756712 Review.
Cited by
-
Variation in missed doses and reasons for discontinuation of anti-tuberculosis drugs during hospital treatment for drug-resistant tuberculosis in South Africa.PLoS One. 2023 Feb 13;18(2):e0281097. doi: 10.1371/journal.pone.0281097. eCollection 2023. PLoS One. 2023. PMID: 36780443 Free PMC article.
-
Is tuberculosis patients management improved in the integrated TB control model in West China? A survey in Guizhou Province, China.Infect Dis Poverty. 2019 Jul 2;8(1):55. doi: 10.1186/s40249-019-0563-3. Infect Dis Poverty. 2019. PMID: 31262368 Free PMC article.
-
Enhancing programmatic scale-up: Applying the consolidated framework for implementation research to evaluate decentralized drug-resistant tuberculosis services in Southern Nigeria.PLoS One. 2025 Feb 21;20(2):e0318274. doi: 10.1371/journal.pone.0318274. eCollection 2025. PLoS One. 2025. PMID: 39982952 Free PMC article.
-
Clinical application of whole-genome sequencing in the management of extensively drug-resistant tuberculosis: a case report.Ann Clin Microbiol Antimicrob. 2024 Aug 22;23(1):76. doi: 10.1186/s12941-024-00737-9. Ann Clin Microbiol Antimicrob. 2024. PMID: 39175078 Free PMC article.
-
Malnutrition and unsuccessful tuberculosis treatment among people with multi-drug resistant tuberculosis in Uganda: A retrospective analysis.J Clin Tuberc Other Mycobact Dis. 2024 Aug 12;37:100477. doi: 10.1016/j.jctube.2024.100477. eCollection 2024 Dec. J Clin Tuberc Other Mycobact Dis. 2024. PMID: 39224115 Free PMC article.
References
-
- WHO . Global tuberculosis report 2015. 20. Geneva: World Health Organization; 2015.
-
- Geerligs WA, Van Altena R, De Lange WCM, Van Soolingen D, Van Der Werf TS. Multidrug-resistant tuberculosis: long term treatment outcome in the Netherlands. Int J Tuberc Lung Dis. 2000;4:758–764. - PubMed
-
- Gupta R, Cegielski JP, Espinal MA, Henkens M, Kim JY, Lambregts-Van Weezenbeek CS, Lee JW, Raviglione MC, Suarez PG, Varaine F. Increasing transparency in partnerships for health—introducing the Green Light Committee. Trop Med Int Health. 2002;7(11):970–976. doi: 10.1046/j.1365-3156.2002.00960.x. - DOI - PubMed
-
- Heller T, Lessells RJ, Wallrauch CG, Bärnighausen T, Cooke GS, Mhlongo L, Master I, Newell ML. Community-based treatment for multidrug-resistant tuberculosis in rural KwaZulu-Natal, South Africa. Int J Tuberc Lung Dis. 2010;14(4):420–426. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
