

Process evaluation of the systematic medical appraisal, referral and treatment (SMART) mental health project in rural India
- PMID: 29202773
- PMCID: PMC5715622
- DOI: 10.1186/s12888-017-1525-6
Process evaluation of the systematic medical appraisal, referral and treatment (SMART) mental health project in rural India
Abstract
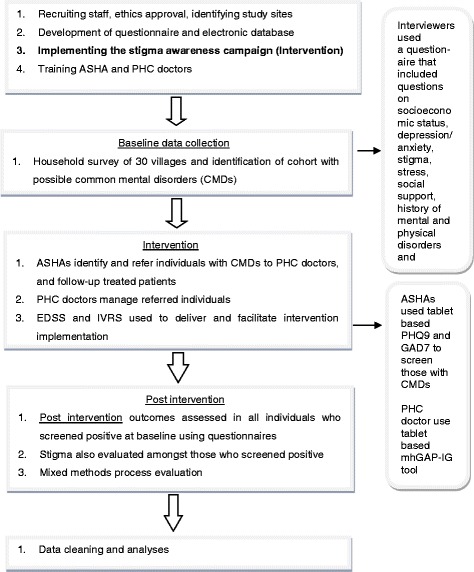
Background: Availability of basic mental health services is limited in rural areas of India. Health system and individual level factors such as lack of mental health professionals and infrastructure, poor awareness about mental health, stigma related to help seeking, are responsible for poor awareness and use of mental health services. We implemented a mental health services delivery model that leveraged technology and task sharing to facilitate identification and treatment of common mental disorders (CMDs) such as stress, depression, anxiety and suicide risk in rural areas of the state of Andhra Pradesh, India. The intervention was delivered by lay village health workers (Accredited Social Health Activists - ASHAs) and primary care doctors. An anti-stigma campaign was implemented prior to this activity. This paper reports the process evaluation of the intervention using mixed methods.
Methods: A mixed methods pre-post evaluation assessed the intervention using quantitative service usage analytics from the server, and qualitative interviews with different stakeholders. Barriers and facilitators in implementing the intervention were identified.
Results: Health service use increased significantly at post-intervention, ASHAs could followup 78.6% of those who had screened positive, and 78.6% of the 1243 Interactive Voice Response System calls made, were successful. Most respondents were aware of the intervention. They indicated that knowledge received through the intervention empowered them to approach ASHAs and share their mental health symptoms. ASHAs and doctors opined that EDSS was useful and easy to use. Medical camps organized in villages to increase access to the doctor were received positively by all. However, some aspects or facilitators of the intervention need to be improved, including network connectivity, booster training, anti-stigma campaigns, quality of mental health services provided by doctors, provision of psychotropic medications at primary health centers and frequency of health camps.
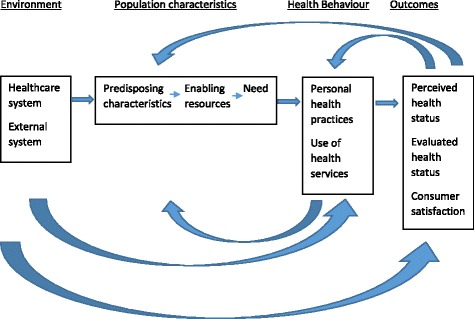
Conclusion: The respondents' views helped to understand the barriers and facilitators for improving the likely effectiveness of the intervention using Andersen's Modified Behavioral Model of Health Services Use, and identify the mechanisms by which those factors affected mental health services uptake in the community.
Trial registration: The study is registered with Clinical Trials Registry India (Applied - 16/07/14-Ref2014/07/007256; registration received - 04/10/17-CTRI/2017/10/009992 ).
Keywords: Common mental disorders; India; Low and middle income countries; Mental health services; Process evaluation; mHealth based interventions.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from the Independent Ethics Committee of the Centre for Chronic Disease Control, New Delhi. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Informed written consent was obtained from all participants.
Consent for publication
Not Applicable.
Competing interests
None of the authors have any competing interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- GBD 2013 DALYs and HALE Collaborators Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet. 2015;386:2145–2191. doi: 10.1016/S0140-6736(15)61340-X. - DOI - PMC - PubMed
-
- World Health Organization . The world health report 2001- mental health: new understanding, new hope. WHO. Switzerland: Geneva; 2001.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
