

Studying de-implementation in health: an analysis of funded research grants
- PMID: 29202782
- PMCID: PMC5715998
- DOI: 10.1186/s13012-017-0655-z
Studying de-implementation in health: an analysis of funded research grants
Abstract
Background: Studying de-implementation-defined herein as reducing or stopping the use of a health service or practice provided to patients by healthcare practitioners and systems-has gained traction in recent years. De-implementing ineffective, unproven, harmful, overused, inappropriate, and/or low-value health services and practices is important for mitigating patient harm, improving processes of care, and reducing healthcare costs. A better understanding of the state-of-the-science is needed to guide future objectives and funding initiatives. To this end, we characterized de-implementation research grants funded by the United States (US) National Institutes of Health (NIH) and the Agency for Healthcare Research and Quality (AHRQ).
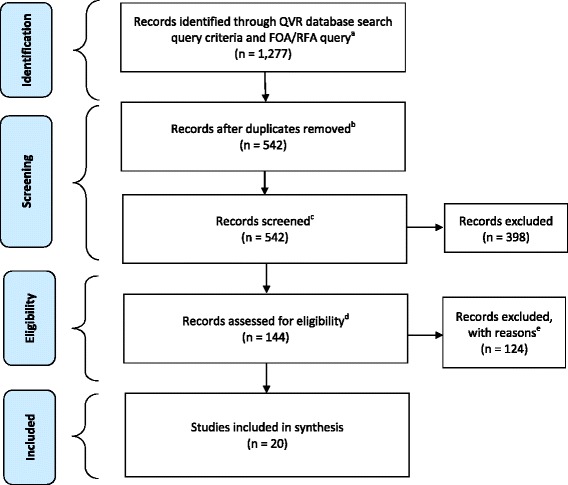
Methods: We used systematic methods to search, identify, and describe de-implementation research grants funded across all 27 NIH Institutes and Centers (ICs) and AHRQ from fiscal year 2000 through 2017. Eleven key terms and three funding opportunity announcements were used to search for research grants in the NIH Query, View and Report (QVR) system. Two coders identified eligible grants based on inclusion/exclusion criteria. A codebook was developed, pilot tested, and revised before coding the full grant applications of the final sample.
Results: A total of 1277 grants were identified through the QVR system; 542 remained after removing duplicates. After the multistep eligibility assessment and review process, 20 grant applications were coded. Many grants were funded by NIH (n = 15), with fewer funded by AHRQ, and a majority were funded between fiscal years 2015 and 2016 (n = 11). Grant proposals focused on de-implementing a range of health services and practices (e.g., medications, therapies, screening tests) across various health areas (e.g., cancer, cardiovascular disease) and delivery settings (e.g., hospitals, nursing homes, schools). Grants proposed to use a variety of study designs and research methods (e.g., experimental, observational, mixed methods) to accomplish study aims.
Conclusions: Based on the systematic portfolio analysis of NIH- and AHRQ-funded research grants over the past 17 years, relatively few have focused on studying the de-implementation of ineffective, unproven, harmful, overused, inappropriate, and/or low-value health services and practices provided to patients by healthcare practitioners and systems. Strategies for raising the profile and growing the field of research on de-implementation are discussed.
Keywords: De-adoption; De-implementation; De-prescribe; Decrease use; Disincentivize; Disinvestment; Evidence-based; Exnovation; Implementation research; Implementation science; Low value; Medical reversal; Overuse; Portfolio analysis.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
WEN is on the editorial board for the journal
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
