

Effects of treatment changes on asthma phenotype prevalence and airway neutrophil function
- PMID: 29202821
- PMCID: PMC5715501
- DOI: 10.1186/s12890-017-0511-6
Effects of treatment changes on asthma phenotype prevalence and airway neutrophil function
Abstract
Background: Asthma inflammatory phenotypes are often defined by relative cell counts of airway eosinophils/neutrophils. However, the importance of neutrophilia remains unclear, as does the effect of ICS treatment on asthma phenotypes and airway neutrophil function. The purpose of this study was to assess asthma phenotype prevalence/characteristics in a community setting, and, in a nested preliminary study, determine how treatment changes affect phenotype stability and inflammation, with particular focus on airway neutrophils.
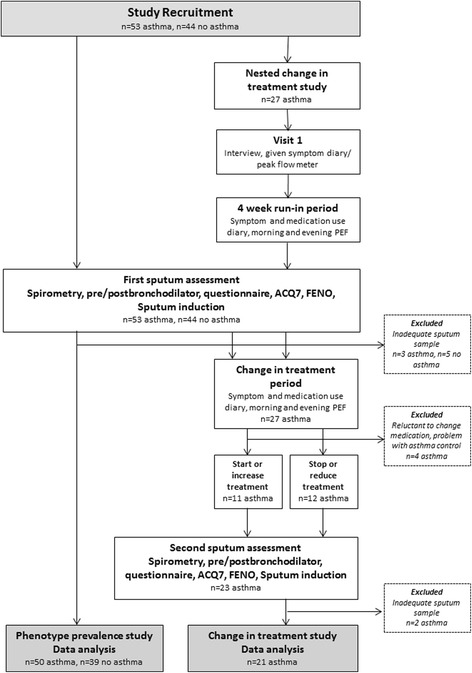
Methods: Fifty adult asthmatics and 39 non-asthmatics were assessed using questionnaires, skin prick tests, spirometry, exhaled nitric oxide (FENO) measurement, and sputum induction. Twenty-one asthmatics underwent further assessment following treatment optimisation (n = 11) or sub-optimisation (n = 10).
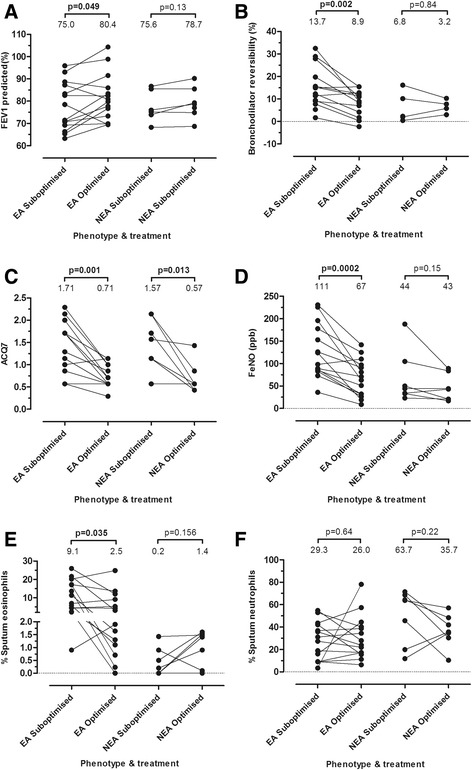
Results: Forty percent (20/50) had eosinophilic asthma (EA) and 8% had neutrophilic asthma. EA was associated with increased FENO, bronchodilator reversibility (BDR) and reduced lung function (p < 0.05). Following optimisation/sub-optimisation, the EA/NEA (non-eosinophilic asthma) phenotype changed in 11/21 (52%) asthmatics. In particular, fewer subjects had EA post treatment optimisation, but this was not statistically significant. However, a significant (p < 0.05) reduction in FENO, ACQ7 score, and BDR was observed after treatment optimisation, as well as an increase in FEV1-% predicted (p < 0.05). It was also associated with reduced eosinophils (p < 0.05) and enhanced neutrophil phagocytosis (p < 0.05) in EA only, and enhanced neutrophil oxidative burst in both EA and NEA (p < 0.05).
Conclusions: In this community based population, non-eosinophilic asthma was common, less severe than EA, and at baseline most asthmatics showed no evidence of inflammation. In the nested change in treatment study, treatment optimisation was associated with reduced sputum eosinophils, improved symptoms and lung function, and enhanced neutrophil function, but a significant reduction in EA could not be demonstrated.
Trial registration: The nested change in treatment component of this study is registered at the Australia and New Zealand Clinical Trial Registry ( www.ANZCTR.org.au ) ACTRN12617001356358 . Registration date 27/09/2017. Retrospectively registered.
Keywords: Asthma; Eosinophils; Induced sputum; Inflammatory phenotype; Neutrophils.
Conflict of interest statement
Ethics approval and consent to participate
The study was performed in accordance with the Declaration of Helsinki and approved by the Upper South A and Lower South Regional Ethics Committee, New Zealand (URA/08/08/056 and LRS/10/07/031 respectively). All subjects gave written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Effects of steroid therapy on inflammatory cell subtypes in asthma.Thorax. 2010 May;65(5):384-90. doi: 10.1136/thx.2009.126722. Epub 2009 Dec 8. Thorax. 2010. PMID: 19996343
-
Albuterol inhalation increases FeNO level in steroid-naive asthmatics but not COPD patients with reversibility.Clin Respir J. 2017 May;11(3):328-336. doi: 10.1111/crj.12340. Epub 2015 Jul 8. Clin Respir J. 2017. PMID: 26077165
-
Relationships among bronchodilator reversibility, the fraction of exhaled nitric oxide, and the parameters of the forced oscillation technique in adult asthma treated with inhaled corticosteroids and long-acting β2 agonists combination.J Breath Res. 2020 Mar 31;14(2):026013. doi: 10.1088/1752-7163/ab7b8c. J Breath Res. 2020. PMID: 32120351
-
Tailoring asthma treatment on eosinophilic markers (exhaled nitric oxide or sputum eosinophils): a systematic review and meta-analysis.Thorax. 2018 Dec;73(12):1110-1119. doi: 10.1136/thoraxjnl-2018-211540. Epub 2018 Jun 1. Thorax. 2018. PMID: 29858277
-
Noninvasive monitoring of airway inflammation and steroid reduction in children with asthma.Curr Opin Allergy Clin Immunol. 2006 Jun;6(3):155-60. doi: 10.1097/01.all.0000225152.37403.21. Curr Opin Allergy Clin Immunol. 2006. PMID: 16670506 Review.
Cited by
-
Association between Childhood Asthma Control Test scores and lung pathophysiologic indicators in longitudinal measurements.J Thorac Dis. 2023 Aug 31;15(8):4207-4215. doi: 10.21037/jtd-22-1383. Epub 2023 Jul 28. J Thorac Dis. 2023. PMID: 37691677 Free PMC article.
-
Weighted gene co-expression network analysis to identify key modules and hub genes associated with paucigranulocytic asthma.BMC Pulm Med. 2021 Nov 2;21(1):343. doi: 10.1186/s12890-021-01711-3. BMC Pulm Med. 2021. PMID: 34727921 Free PMC article.
-
Enhanced airway sensory nerve reactivity in non-eosinophilic asthma.BMJ Open Respir Res. 2021 Nov;8(1):e000974. doi: 10.1136/bmjresp-2021-000974. BMJ Open Respir Res. 2021. PMID: 34728474 Free PMC article.
-
Understanding asthma phenotypes: the World Asthma Phenotypes (WASP) international collaboration.ERJ Open Res. 2018 Aug 22;4(3):00013-2018. doi: 10.1183/23120541.00013-2018. eCollection 2018 Jul. ERJ Open Res. 2018. PMID: 30151371 Free PMC article.
-
Human PD-1 agonist treatment alleviates neutrophilic asthma by reprogramming T cells.J Allergy Clin Immunol. 2023 Feb;151(2):526-538.e8. doi: 10.1016/j.jaci.2022.07.022. Epub 2022 Aug 11. J Allergy Clin Immunol. 2023. PMID: 35963455 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
