

Electronic medical records can be used to emulate target trials of sustained treatment strategies
- PMID: 29203418
- PMCID: PMC5847447
- DOI: 10.1016/j.jclinepi.2017.11.021
Electronic medical records can be used to emulate target trials of sustained treatment strategies
Abstract
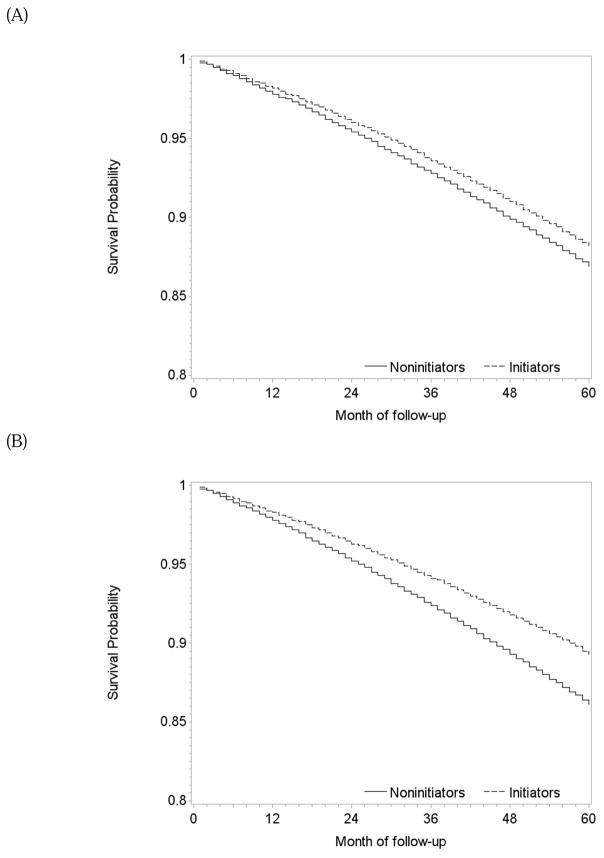
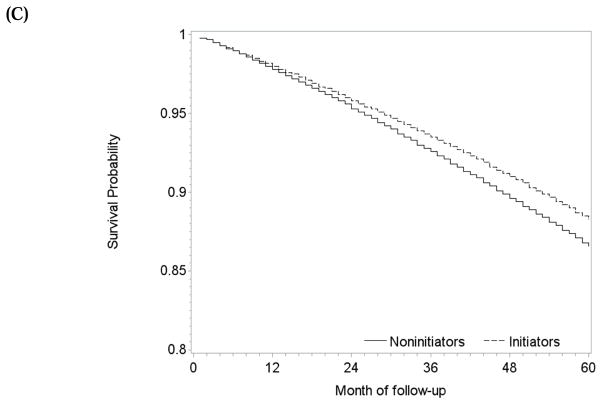
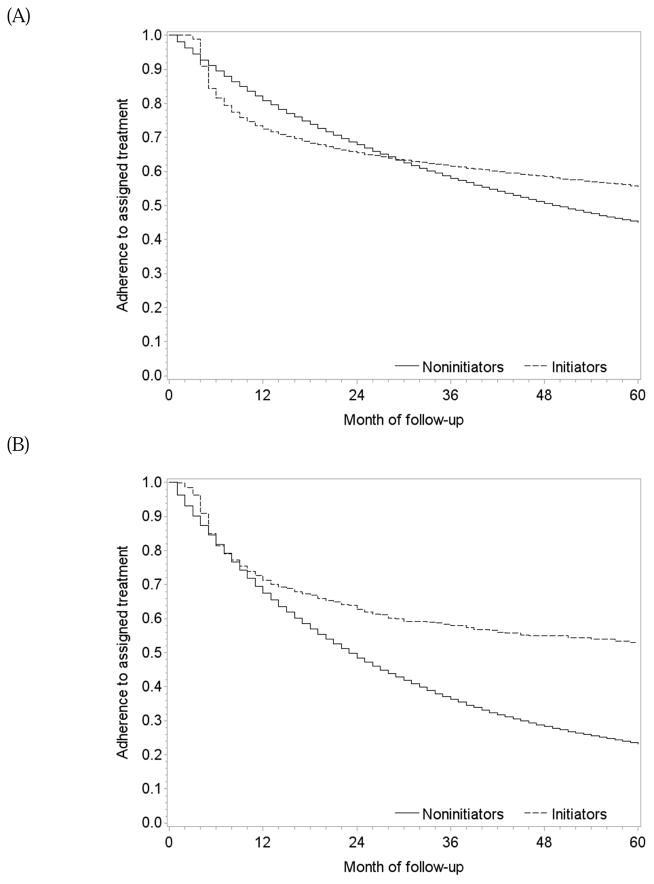
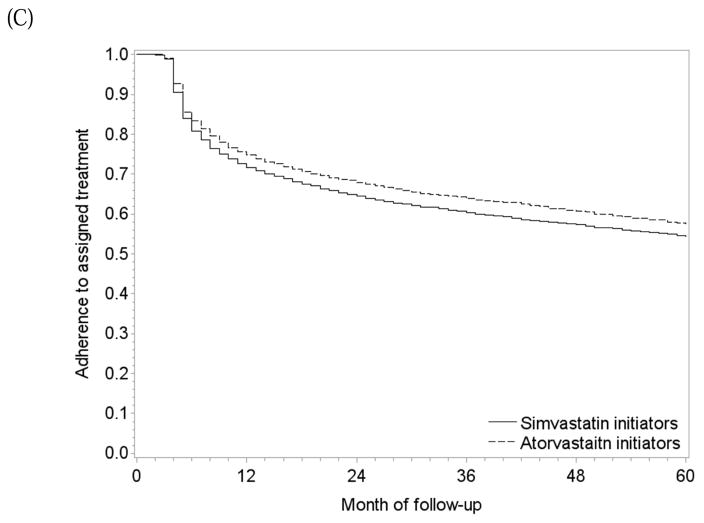
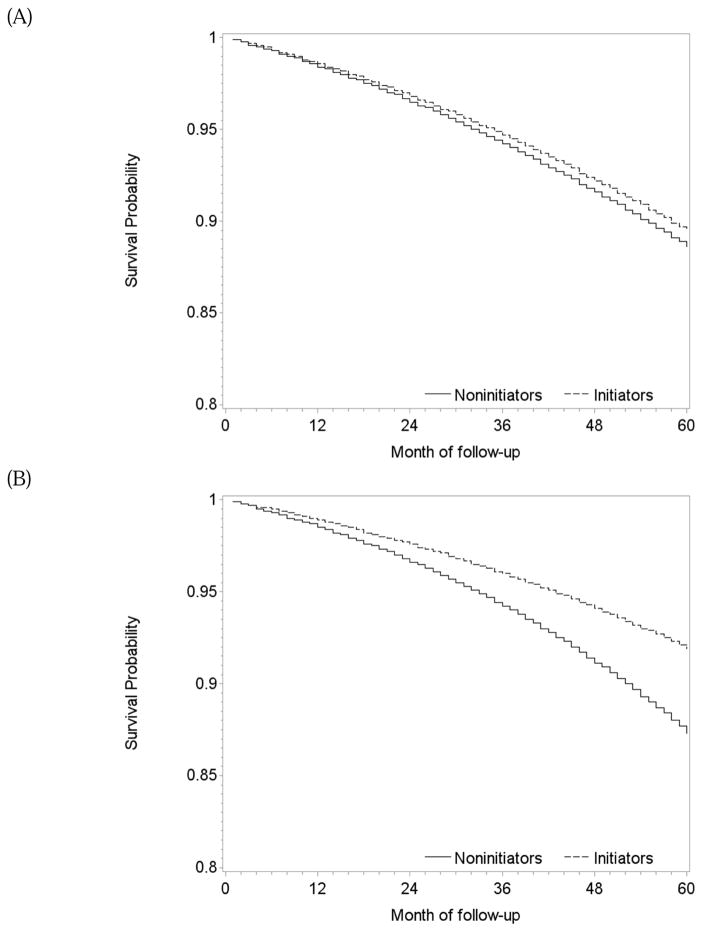
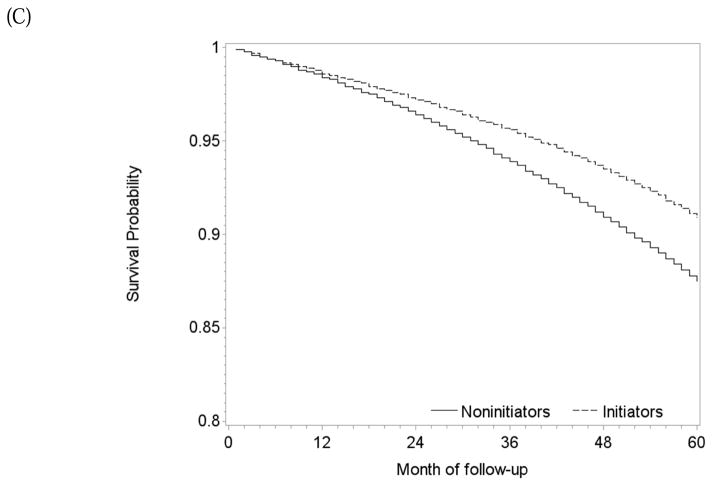
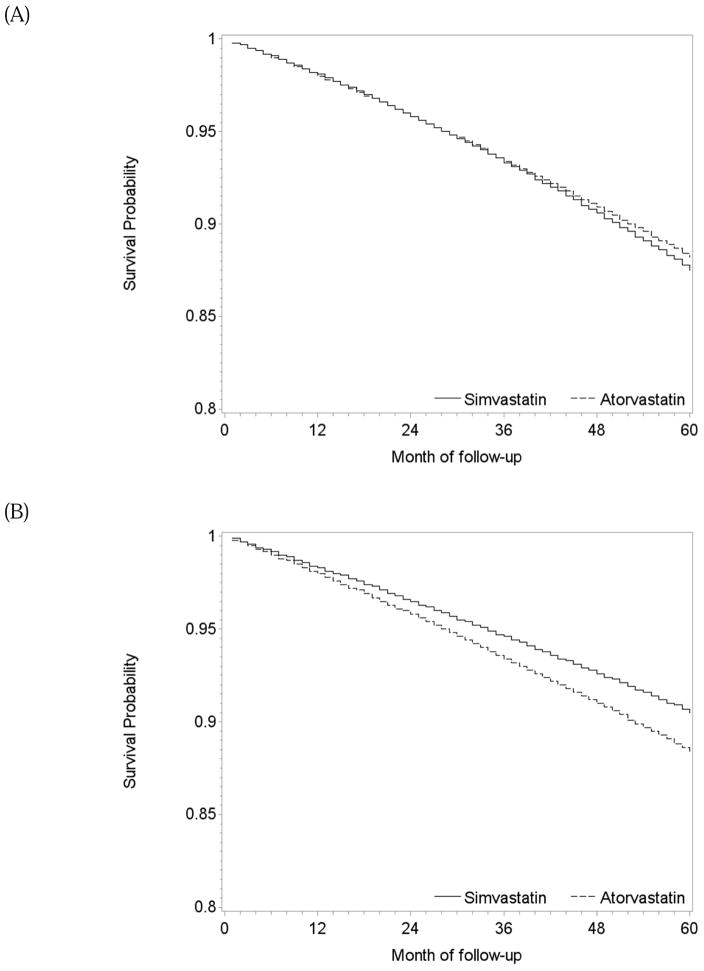
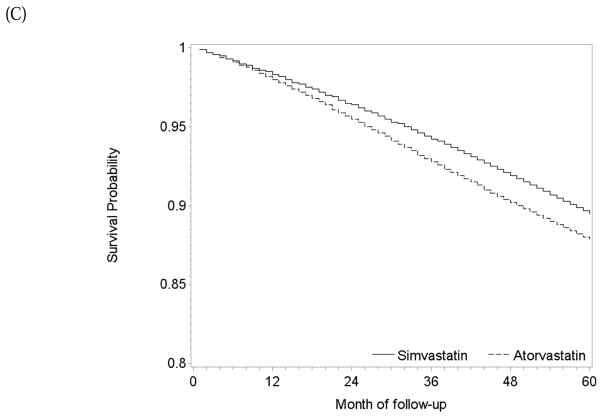
Objective: To emulate three target trials: single treatment vs. no treatment, joint treatment vs. no treatment, and head-to-head comparison of two treatments, we explain how to estimate the observational analogs of intention-to-treat and per-protocol effects, using hazard ratios and survival curves. For per-protocol effects, we describe two methods for adherence adjustment via inverse-probability weighting.
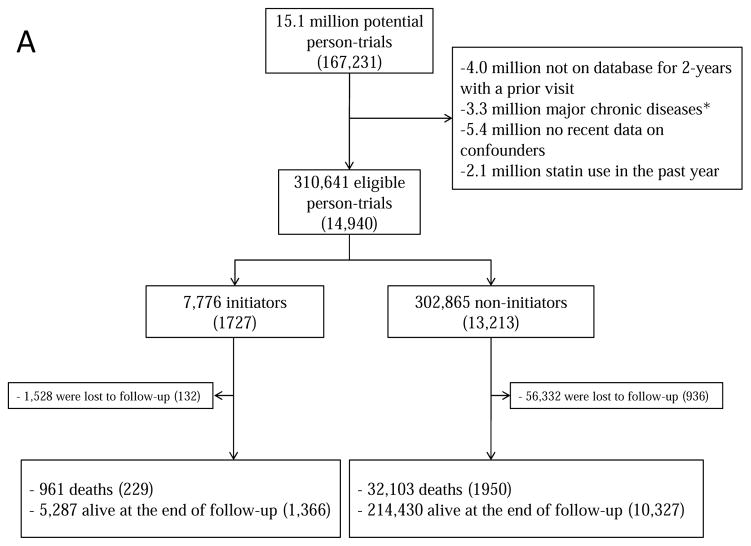
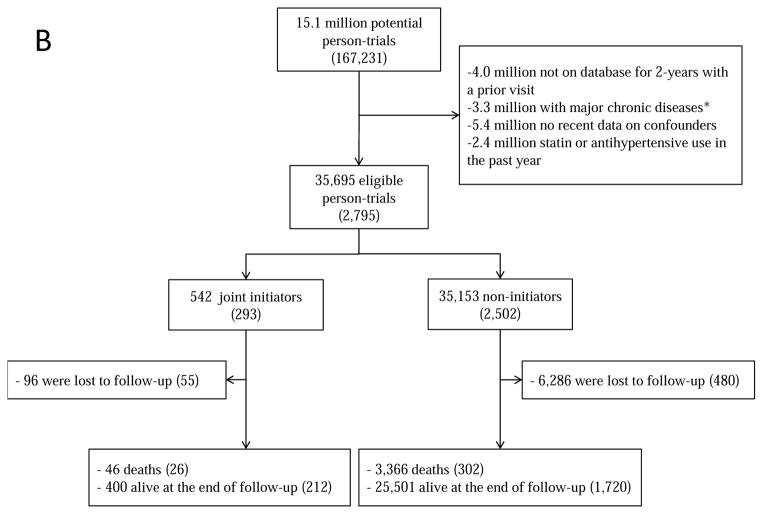
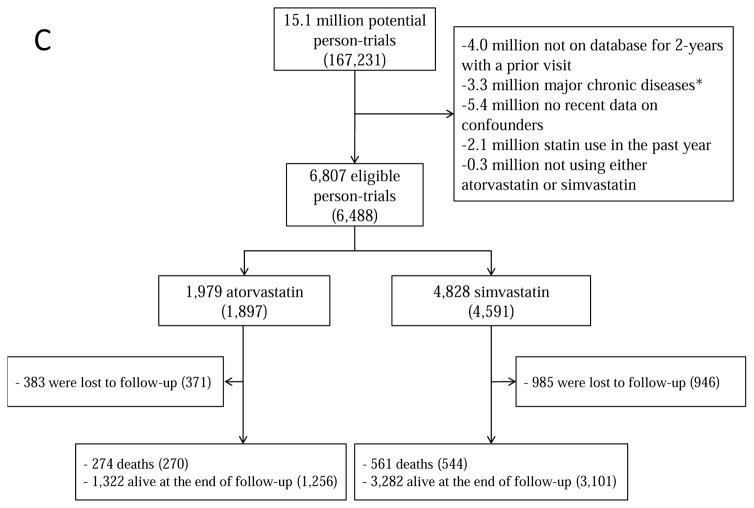
Study design and setting: Prospective observational study using electronic medical records of individuals aged 55-84 with coronary heart disease from >500 practices in the United Kingdom between 2000 and 2010.
Results: The intention-to-treat mortality hazard ratio (95% confidence interval) was 0.90 (0.84, 0.97) for statins vs. no treatment, 0.88 (0.73, 1.06) for statins plus antihypertensives vs. no treatment, and 0.91 (0.77, 1.06) for atorvastatin vs. simvastatin. When censoring nonadherent person-times, the per-protocol mortality hazard ratio was 0.74 (0.64, 0.85) for statins vs. no treatment, 0.55 (0.35, 0.87) for statins plus antihypertensives vs. no treatment, and 1.13 (0.88, 1.45) for atorvastatin vs. simvastatin. We estimated per-protocol hazard ratios for a 5-year treatment using different dose-response marginal structural models and standardized survival curves for each target trial using intention-to-treat and per-protocol analyses.
Conclusion: When randomized trials are not available or feasible, observational analyses can emulate a variety of target trials.
Keywords: Comparative effectiveness; Confounding; Electronic health records; Medication adherence; Secondary prevention; Survival analysis.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Statins and risk of diabetes: an analysis of electronic medical records to evaluate possible bias due to differential survival.Diabetes Care. 2013 May;36(5):1236-40. doi: 10.2337/dc12-1756. Epub 2012 Dec 17. Diabetes Care. 2013. PMID: 23248196 Free PMC article.
-
Observational data for comparative effectiveness research: an emulation of randomised trials of statins and primary prevention of coronary heart disease.Stat Methods Med Res. 2013 Feb;22(1):70-96. doi: 10.1177/0962280211403603. Epub 2011 Oct 19. Stat Methods Med Res. 2013. PMID: 22016461 Free PMC article.
-
A comparison of secondary prevention practice in poststroke and coronary heart disease patients.Public Health. 2016 Aug;137:64-72. doi: 10.1016/j.puhe.2016.02.003. Epub 2016 Mar 17. Public Health. 2016. PMID: 26996311
-
Developing New Methods for Comparing Treatments in Case-Control Studies [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jul. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jul. PMID: 38976621 Free Books & Documents. Review.
-
Are statins created equal? Evidence from randomized trials of pravastatin, simvastatin, and atorvastatin for cardiovascular disease prevention.Am Heart J. 2006 Feb;151(2):273-81. doi: 10.1016/j.ahj.2005.04.003. Am Heart J. 2006. PMID: 16442888 Review.
Cited by
-
Association of a Shortened Duration of Adjuvant Chemotherapy With Overall Survival Among Individuals With Stage III Colon Cancer.JAMA Netw Open. 2021 Mar 1;4(3):e213587. doi: 10.1001/jamanetworkopen.2021.3587. JAMA Netw Open. 2021. PMID: 33783516 Free PMC article.
-
Emulating a target trial of statin use and risk of dementia using cohort data.Neurology. 2020 Sep 8;95(10):e1322-e1332. doi: 10.1212/WNL.0000000000010433. Epub 2020 Aug 4. Neurology. 2020. PMID: 32753444 Free PMC article.
-
Hypothetical blood-pressure-lowering interventions and risk of stroke and dementia.Eur J Epidemiol. 2021 Jan;36(1):69-79. doi: 10.1007/s10654-020-00694-5. Epub 2020 Nov 27. Eur J Epidemiol. 2021. PMID: 33247419 Free PMC article.
-
Estimating the effect of nutritional interventions using observational data: the American Heart Association's 2020 Dietary Goals and mortality.Am J Clin Nutr. 2021 Aug 2;114(2):690-703. doi: 10.1093/ajcn/nqab100. Am J Clin Nutr. 2021. PMID: 34041538 Free PMC article.
-
Protocol for LINKS (linking individual needs to community and clinical services): a prospective matched observational study of a community health worker community clinical linkage intervention on the U.S.-Mexico border.BMC Public Health. 2019 Apr 11;19(1):399. doi: 10.1186/s12889-019-6725-1. BMC Public Health. 2019. PMID: 30975126 Free PMC article.
References
-
- Avorn J. Debate about funding comparative-effectiveness research. N Engl J Med. 2009;360(19):1927–9. Epub 2009/05/08. - PubMed
-
- Washington AE, Lipstein SH. The Patient-Centered Outcomes Research Institute--promoting better information, decisions, and health. N Engl J Med. 2011;365(15):e31. Epub 2011/10/14. - PubMed
-
- Dreyer NA. Making observational studies count: shaping the future of comparative effectiveness research. Epidemiology. 2011;22(3):295–7. Epub 2011/04/06. - PubMed
-
- Danaei G, Garcia Rodriguez LA, Cantero OF, Logan R, Hernán MA. Observational data for comparative effectiveness research: An emulation of randomised trials of statins and primary prevention of coronary heart disease. Statistical methods in medical research. 2013;22(1):70–96. Epub 2011/10/22. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
