

Comparison of adverse events rates and hospital cost between customized individually made implants and standard off-the-shelf implants for total knee arthroplasty
- PMID: 29204493
- PMCID: PMC5712025
- DOI: 10.1016/j.artd.2017.05.001
Comparison of adverse events rates and hospital cost between customized individually made implants and standard off-the-shelf implants for total knee arthroplasty
Abstract
Background: This study compares selected hospital outcomes between patients undergoing total knee arthroplasty (TKA) using either a customized individually made (CIM) implant or a standard off-the-shelf (OTS) implant.
Methods: A retrospective review was conducted on 248 consecutive TKA patients treated in a single institution, by the same surgeon. Patients received either CIM (126) or OTS (122) implants. Study data were collected from patients' medical record or the hospital's administrative billing record. Standard statistical methods tested for differences in selected outcome measures between the 2 study arms.
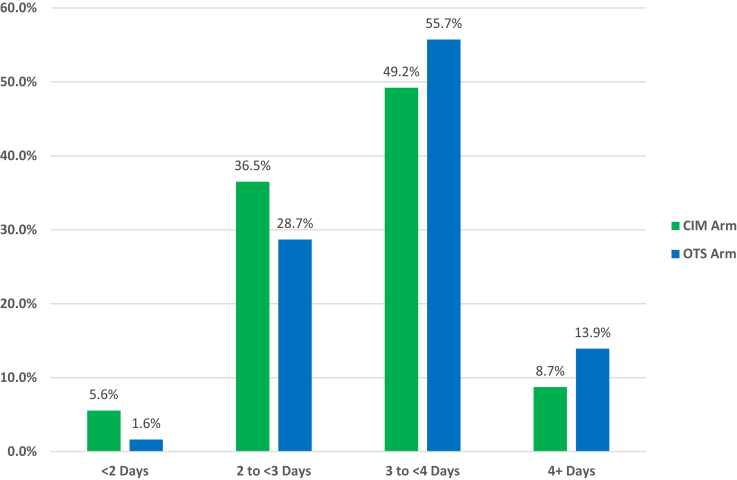
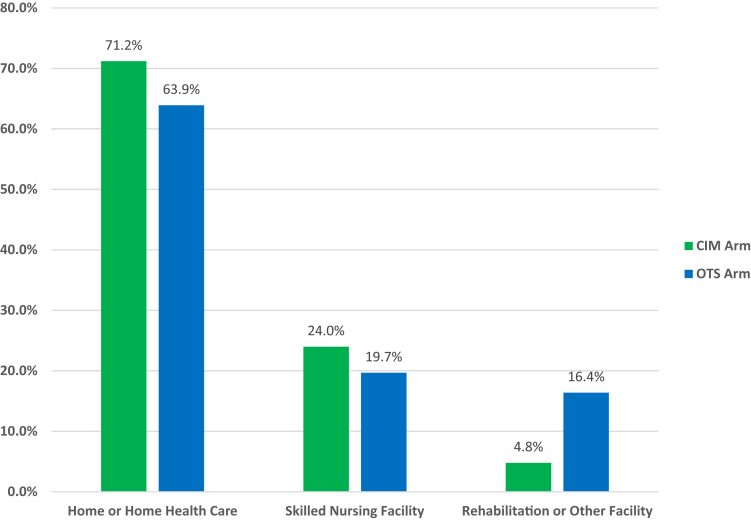
Results: Compared with the OTS implant study arm, the CIM implant study arm showed significantly lower transfusion rates (2.4% vs 11.6%; P = .005); a lower adverse event rate at both discharge (CIM 3.3% vs OTS 14.1%; P = .003) and 90 days after discharge (CIM 8.1% vs OTS 18.2%; P = .023); and a smaller percentage of patients were discharged to a rehabilitation or other acute care facility (4.8% vs 16.4%; P = .003). Total average real hospital cost for the TKA hospitalization between the 2 groups were nearly identical (CIM $16,192 vs OTS $16,240; P = .913). Finally, the risk-adjusted per patient total cost of care showed a net savings of $913.87 (P = .240) per patient for the CIM-TKA group, for bundle of care including the preoperative computed tomography scan, TKA hospitalization, and discharge disposition.
Conclusions: Patients treated with a CIM implant had significantly lower transfusion rates, fewer adverse event rates, and were less likely to be discharged to a rehabilitation facility or another acute care facility. These outcomes were achieved without increasing costs.
Keywords: Adverse event rate; Customized individually made implant; Hospital cost; Length of stay; TKA.
Figures
Similar articles
-
In Vivo Tibial Fit and Rotational Analysis of a Customized, Patient-Specific TKA versus Off-the-Shelf TKA.J Knee Surg. 2019 Jun;32(6):499-505. doi: 10.1055/s-0038-1653966. Epub 2018 May 25. J Knee Surg. 2019. PMID: 29801179
-
No difference in patient-reported satisfaction after 12 months between customised individually made and off-the-shelf total knee arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2022 Sep;30(9):2948-2957. doi: 10.1007/s00167-022-06900-z. Epub 2022 Feb 12. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 35149877 Free PMC article.
-
Comparison of Postoperative Coronal Leg Alignment in Customized Individually Made and Conventional Total Knee Arthroplasty.J Pers Med. 2021 Jun 12;11(6):549. doi: 10.3390/jpm11060549. J Pers Med. 2021. PMID: 34204771 Free PMC article.
-
Customised, individually made total knee arthroplasty shows promising 1-year clinical and patient reported outcomes.Arch Orthop Trauma Surg. 2021 Dec;141(12):2217-2225. doi: 10.1007/s00402-021-04045-1. Epub 2021 Jul 16. Arch Orthop Trauma Surg. 2021. PMID: 34269890 Free PMC article. Review.
-
Factors associated with hospital stay length, discharge destination, and 30-day readmission rate after primary hip or knee arthroplasty: Retrospective Cohort Study.Orthop Traumatol Surg Res. 2019 Sep;105(5):949-955. doi: 10.1016/j.otsr.2019.04.012. Epub 2019 Jun 15. Orthop Traumatol Surg Res. 2019. PMID: 31208932 Review.
Cited by
-
Evolution of Titanium Interbody Cages and Current Uses of 3D Printed Titanium in Spine Fusion Surgery.Curr Rev Musculoskelet Med. 2024 Jul 14. doi: 10.1007/s12178-024-09912-z. Online ahead of print. Curr Rev Musculoskelet Med. 2024. PMID: 39003679 Review.
-
Clinical and Economic Case for Patient-Specific Total Knee Arthroplasty: A Prospective Study.Cureus. 2025 Mar 8;17(3):e80270. doi: 10.7759/cureus.80270. eCollection 2025 Mar. Cureus. 2025. PMID: 40201868 Free PMC article.
-
The Economic Value of Customized versus Off-the-Shelf Knee Implants in Medicare Fee-for-Service Beneficiaries.Am Health Drug Benefits. 2019 Apr;12(2):66-73. Am Health Drug Benefits. 2019. PMID: 31057693 Free PMC article.
-
A pilot study on preferences from surgeons to deal with an innovative customized and connected knee prosthesis - A discret choice experiment.Heliyon. 2024 May 8;10(10):e30041. doi: 10.1016/j.heliyon.2024.e30041. eCollection 2024 May 30. Heliyon. 2024. PMID: 38784553 Free PMC article.
-
A computational tool for automatic selection of total knee replacement implant size using X-ray images.Front Bioeng Biotechnol. 2022 Sep 29;10:971096. doi: 10.3389/fbioe.2022.971096. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36246387 Free PMC article.
References
-
- Kurtz S., Ong K., Lau E., Mowat F., Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780. - PubMed
-
- Gill G.S., Mills D., Joshi A.B. Mortality following primary TKA. J Bone Joint Surg Am. 2003;85(3):432. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
