

Who Is the Patient at Risk of CMV Recurrence: A Review of the Current Scientific Evidence with a Focus on Hematopoietic Cell Transplantation
- PMID: 29204910
- PMCID: PMC5840099
- DOI: 10.1007/s40121-017-0180-z
Who Is the Patient at Risk of CMV Recurrence: A Review of the Current Scientific Evidence with a Focus on Hematopoietic Cell Transplantation
Abstract
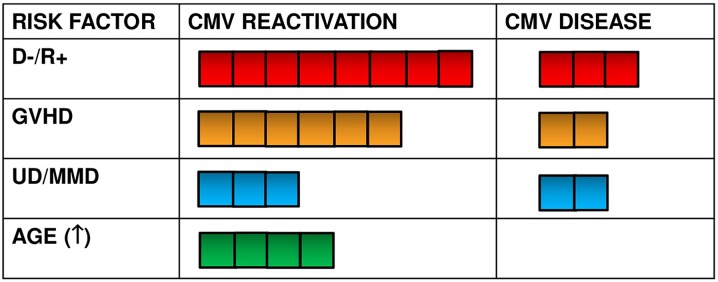
Cytomegalovirus (CMV) is an agent of global infection, and its acquisition in a population is characterized by an age-dependent rise in seropositivity. After primary infection, CMV remains in the host cells in latent form, and it can reactivate in the case of immune suppression. The risk of CMV recurrence is dependent on the level of incompetency of the immune system, manifested as an impairment of T-cell immunity, including the presence and function of CMV-specific cytotoxic T lymphocytes. This article presents data on the incidence of CMV recurrence in groups of immunocompromised patients, including allogeneic hematopoietic stem cell transplantation (HSCT) patients and other groups of patients, based on a summary of reported data. The median rate of CMV recurrence in HSCT recipients was estimated as 37% after allogeneic transplant and 12% after autologous transplant, 5% in patients with nontransplant hematological malignancies, 14% in recipients of anti-CD52 therapy, 30% in solid organ transplant recipients, 21% in patients with primary immunodeficiencies, 20% during active replication in HIV-positive patients and 3.3% during antiretroviral therapy, 7% in patients with chronic kidney disease, 0.6% in patients with congenital infection, and 0.6% in neonates with primary infection. The highest risk of CMV recurrence and CMV disease is reported for HSCT CMV-seropositive recipients, regardless of donor serostatus. The odds ratio (OR) for CMV recurrence is higher for recipient-positive versus recipient-negative CMV serostatus transplants (OR 8.0), donor-negative/recipient-positive versus donor-positive/recipient-positive CMV serostatus transplants (OR 1.2), unrelated/mismatched versus matched-family donor transplants (OR 1.6), and acute graft-versus-host-disease versus other diseases (OR 3.2). Other risk factors have minor significance.
Keywords: Cytomegalovirus; Cytomegalovirus disease; Cytomegalovirus recurrence; Hematopoietic stem cell transplantation; Population; Risk factors; Risk group.
Figures

References
-
- Styczynski J. Managing post-transplant lymphoproliferative disorder. Expert Opin Orphan Drugs. 2017;5(1):19–35. doi: 10.1080/21678707.2017.1262256. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
