

Systemic Markers of Adaptive and Innate Immunity Are Associated with Chronic Obstructive Pulmonary Disease Severity and Spirometric Disease Progression
- PMID: 29206476
- PMCID: PMC5894501
- DOI: 10.1165/rcmb.2017-0373OC
Systemic Markers of Adaptive and Innate Immunity Are Associated with Chronic Obstructive Pulmonary Disease Severity and Spirometric Disease Progression
Abstract
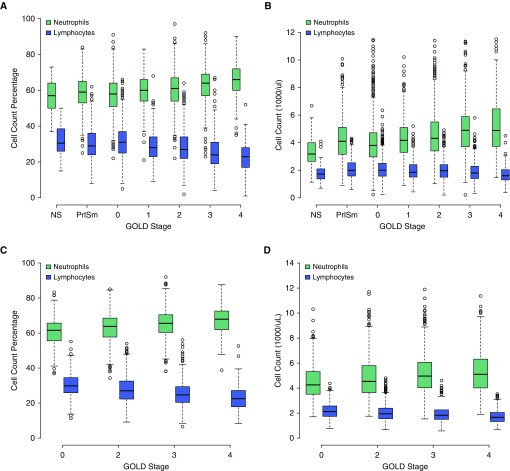
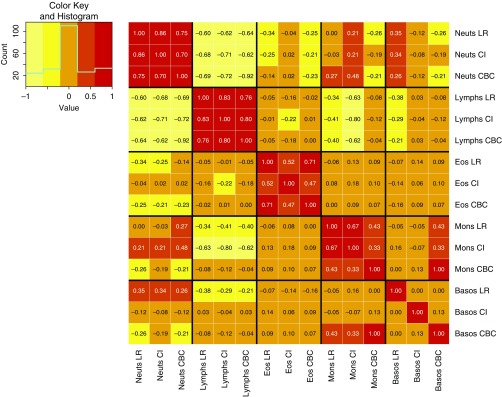
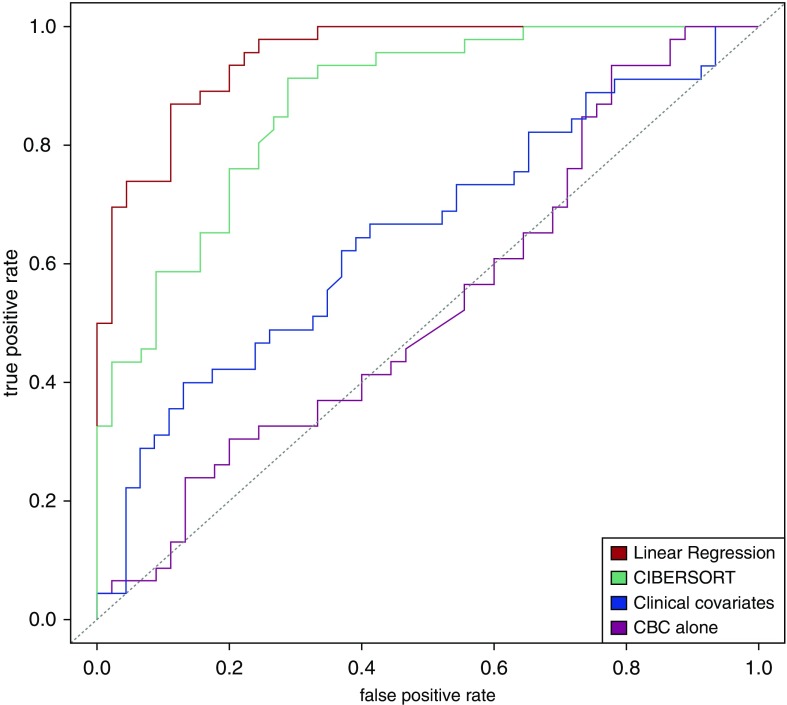
The progression of chronic obstructive pulmonary disease (COPD) is associated with marked alterations in circulating immune cell populations, but no studies have characterized alterations in these cell types across the full spectrum of lung function impairment in current and former smokers. In 6,299 subjects from the COPDGene and ECLIPSE (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints) studies, we related Coulter blood counts and proportions to cross-sectional forced expiratory volume in 1 second (FEV1), adjusting for current smoking status. We also related cell count measures to 3-year change in FEV1 in ECLIPSE subjects. In a subset of subjects with blood gene expression data, we used cell type deconvolution methods to infer the proportions of immune cell subpopulations, and we related these to COPD clinical status. We observed that FEV1 levels are positively correlated with lymphocytes and negatively correlated with myeloid populations, such as neutrophils and monocytes. In multivariate models, absolute cell counts and proportions were associated with cross-sectional FEV1, and lymphocytes, monocytes, and eosinophil counts were predictive of 3-year change in lung function. Using cell type deconvolution to study immune cell subpopulations, we observed that subjects with COPD had a lower proportion of CD4+ resting memory cells and naive B cells compared with smokers without COPD. Alterations in circulating immune cells in COPD support a mixed pattern of lymphocyte suppression and an enhanced myeloid cell immune response. Cell counts and proportions contribute independent information to models predicting lung function, suggesting a critical role for immune response in long-term COPD outcomes. Cell type deconvolution is a promising method for immunophenotyping in large cohorts.
Trial registration: ClinicalTrials.gov NCT00608764.
Keywords: chronic obstructive pulmonary disease; computational biology; gene expression; immunology.
Figures
References
-
- Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33:1165–1185. - PubMed
-
- Sapey E, Stockley JA, Greenwood H, Ahmad A, Bayley D, Lord JM, et al. Behavioral and structural differences in migrating peripheral neutrophils from patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;183:1176–1186. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
