

Advance Care Planning in an Accountable Care Organization Is Associated with Increased Advanced Directive Documentation and Decreased Costs
- PMID: 29206564
- PMCID: PMC5867515
- DOI: 10.1089/jpm.2017.0566
Advance Care Planning in an Accountable Care Organization Is Associated with Increased Advanced Directive Documentation and Decreased Costs
Abstract
Background: Advance care planning (ACP) documents patient wishes and increases awareness of palliative care options.
Objective: To study the association of outpatient ACP with advanced directive documentation, utilization, and costs of care.
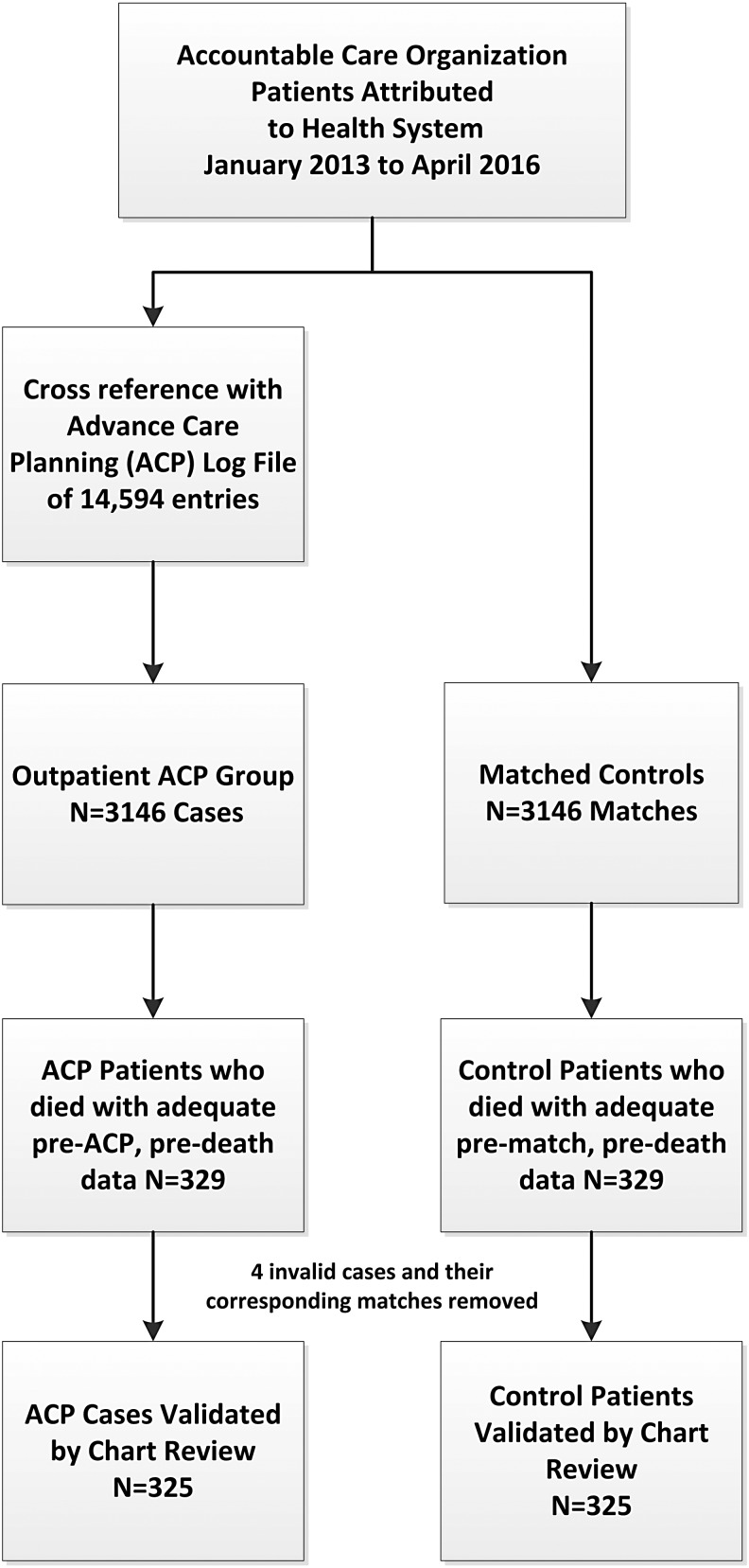
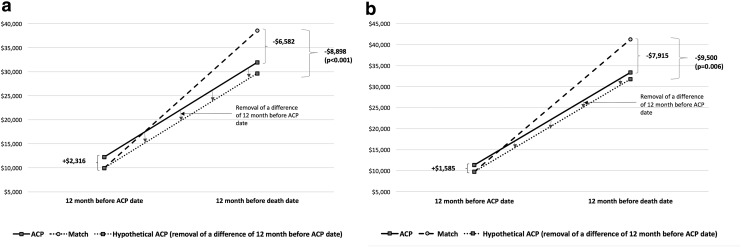
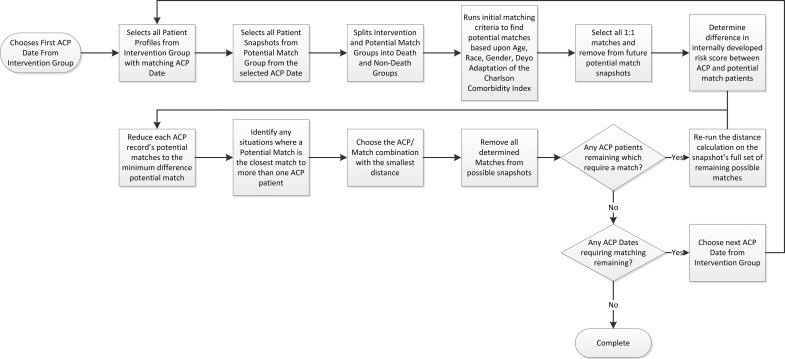
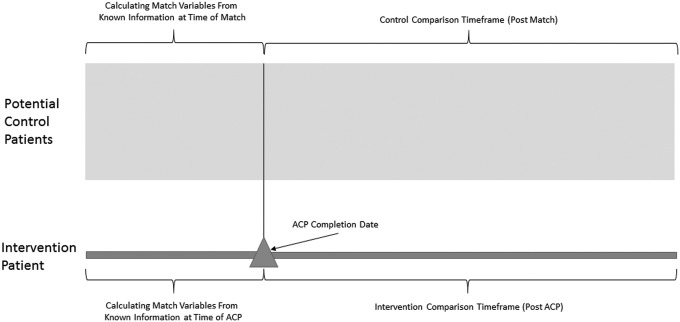
Design: This was a case-control study of cases with ACP who died matched 1:1 with controls. We used 12 months of data pre-ACP/prematch and predeath. We compared rates of documentation with logit model regression and conducted a difference-in-difference analysis using generalized linear models for utilization and costs.
Setting/subjects: Medicare beneficiaries attributed to a large rural-suburban-small metro multisite accountable care organization from January 2013 to April 2016, with cross reference to ACP facilitator logs to find cases.
Measurements: The presence of advance directive forms was verified by chart review. Cost analysis included all utilization and costs billed to Medicare.
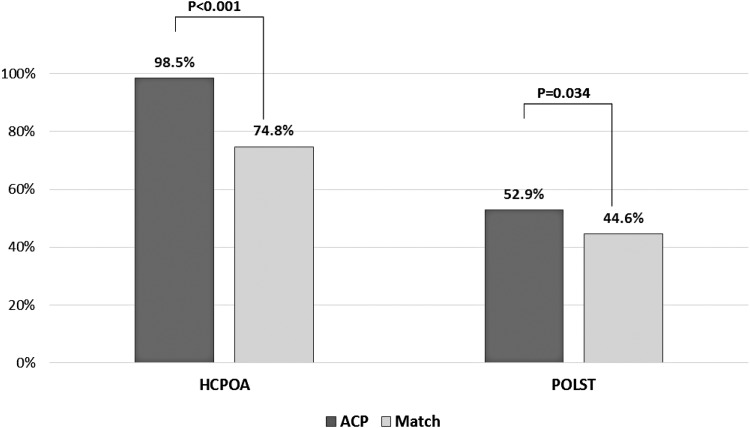
Results: We matched 325 cases and 325 controls (51.1% female and 48.9% male, mean age 81). 320/325 (98.5%) ACP versus 243/325 (74.8%) of controls had a Healthcare Power of Attorney (odds ratio [OR] 21.6, 95% CI 8.6-54.1) and 172/325(52.9%) ACP versus 145/325 (44.6%) controls had Practitioner Orders for Life Sustaining Treatment (OR 1.40, 95% CI 1.02-1.90) post-ACP/postmatch. Adjusted results showed ACP cases had fewer inpatient admissions (-0.37 admissions, 95% CI -0.66 to -0.08), and inpatient days (-3.66 days, 95% CI -6.23 to -1.09), with no differences in hospice, hospice days, skilled nursing facility use, home health use, 30-day readmissions, or emergency department visits. Adjusted costs were $9,500 lower in the ACP group (95% CI -$16,207 to -$2,793).
Conclusions: ACP increases documentation and was associated with a reduction in overall costs driven primarily by a reduction in inpatient utilization. Our data set was limited by small numbers of minorities and cancer patients.
Keywords: advance care planning; advance directives; healthcare costs; healthcare power of attorney; healthcare utilization; practitioner orders for life sustaining treatment.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- IOM (Institute of Medicine): Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life. Washington, DC: The National Academies Press, 2014 - PubMed
-
- Penrod JD, Deb P, Luhrs C, et al. : Cost and utilization outcomes of patients receiving hospital-based palliative care consultation. J Palliat Med 2006;9:855–860 - PubMed
-
- Heyland DK, Barwich D, Pichora D, et al. : FAilure to engage hospitalized elderly patients and their families in advance care planning. JAMA Inter Med 2013;173:778–787 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous