

Viral Drug Resistance Through 48 Weeks, in a Phase 2b, Randomized, Controlled Trial of the HIV-1 Attachment Inhibitor Prodrug, Fostemsavir
- PMID: 29206721
- PMCID: PMC5815643
- DOI: 10.1097/QAI.0000000000001602
Viral Drug Resistance Through 48 Weeks, in a Phase 2b, Randomized, Controlled Trial of the HIV-1 Attachment Inhibitor Prodrug, Fostemsavir
Abstract
Background: Fostemsavir is a prodrug of temsavir, an attachment inhibitor that binds to HIV-1 gp120, blocking viral attachment to host CD4 T-cells. The phase 2b trial AI438011 investigated the safety, efficacy, and dose-response of fostemsavir vs ritonavir-boosted atazanavir (ATV/r) in treatment-experienced, HIV-1-infected subjects.
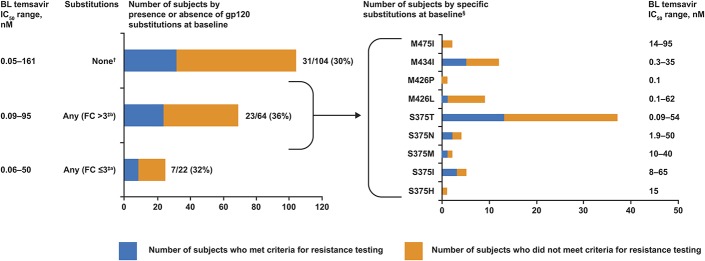
Methods: Two hundred fifty-one treatment-experienced subjects with baseline (BL) susceptibility to study drugs [temsavir half-maximal inhibitory concentration (IC50) <100 nM, PhenoSense Entry assay] received fostemsavir or ATV/r, each with tenofovir disoproxil fumarate + raltegravir. Subjects meeting resistance-testing criteria were assessed for emergent viral drug resistance. Changes in temsavir IC50 from BL was given a conservative technical cutoff (>3-fold increase).
Results: 66/200 fostemsavir and 14/51 ATV/r subjects had resistance testing performed; 44/66 and 9/14 were successfully tested using the PhenoSense GT assay. No subjects had emergent tenofovir disoproxil fumarate or ATV resistance. Six fostemsavir-treated subjects developed emergent raltegravir resistance. 29/66 fostemsavir-treated subjects had an evaluable phenotype using PhenoSense Entry (which tests for viral susceptibility to temsavir) and 13/29 exhibited >3-fold increase in temsavir IC50 from BL. gp120 population sequencing was successful in 11/13 subjects and 7 had emergent substitutions in gp120 associated with reduced temsavir susceptibility (S375, M426, or M434). However, 5/13 fostemsavir-treated subjects achieved subsequent suppression to <50 copies/mL before the week 48 database lock, regardless of key gp120 substitutions.
Conclusions: Response rates remained similar across study arms regardless of BL nucleoside reverse transcriptase inhibitor, nonnucleoside reverse transcriptase inhibitor, and protease inhibitor resistance-associated mutations. Emergent changes in viral susceptibility occurred more frequently with fostemsavir compared with ATV/r. However, the full impact of temsavir IC50 changes and emergent HIV-1 gp120 substitutions, and thus appropriate clinical cutoffs, requires further study. Fostemsavir is being evaluated in a phase 3 trial in heavily treatment-experienced subjects.
Figures
Similar articles
-
Safety and efficacy of the HIV-1 attachment inhibitor prodrug fostemsavir in antiretroviral-experienced subjects: week 48 analysis of AI438011, a Phase IIb, randomized controlled trial.Antivir Ther. 2017;22(3):215-223. doi: 10.3851/IMP3112. Epub 2016 Dec 6. Antivir Ther. 2017. PMID: 27922453 Clinical Trial.
-
Safety and efficacy of the HIV-1 attachment inhibitor prodrug fostemsavir in heavily treatment-experienced individuals: week 96 results of the phase 3 BRIGHTE study.Lancet HIV. 2020 Nov;7(11):e740-e751. doi: 10.1016/S2352-3018(20)30240-X. Lancet HIV. 2020. PMID: 33128903 Clinical Trial.
-
Safety and efficacy of the HIV-1 attachment inhibitor prodrug BMS-663068 in treatment-experienced individuals: 24 week results of AI438011, a phase 2b, randomised controlled trial.Lancet HIV. 2015 Oct;2(10):e427-37. doi: 10.1016/S2352-3018(15)00177-0. Epub 2015 Sep 1. Lancet HIV. 2015. PMID: 26423650 Clinical Trial.
-
Ibalizumab and Fostemsavir in the Management of Heavily Pre-Treated HIV-infected Patients.Recent Pat Antiinfect Drug Discov. 2018;13(3):190-197. doi: 10.2174/1574891X13666181031120019. Recent Pat Antiinfect Drug Discov. 2018. PMID: 30378502 Review.
-
Fostemsavir: First Approval.Drugs. 2020 Sep;80(14):1485-1490. doi: 10.1007/s40265-020-01386-w. Drugs. 2020. PMID: 32852743 Review.
Cited by
-
Susceptibility of global HIV-1 clinical isolates to fostemsavir using the PhenoSense® Entry assay.J Antimicrob Chemother. 2021 Feb 11;76(3):648-652. doi: 10.1093/jac/dkaa474. J Antimicrob Chemother. 2021. PMID: 33241285 Free PMC article.
-
Characterization of Human Immunodeficiency Virus (HIV-1) Envelope Glycoprotein Variants Selected for Resistance to a CD4-Mimetic Compound.J Virol. 2022 Sep 14;96(17):e0063622. doi: 10.1128/jvi.00636-22. Epub 2022 Aug 18. J Virol. 2022. PMID: 35980207 Free PMC article.
-
The Phenomenon of Antiretroviral Drug Resistance in the Context of Human Immunodeficiency Virus Treatment: Dynamic and Ever Evolving Subject Matter.Biomedicines. 2024 Apr 20;12(4):915. doi: 10.3390/biomedicines12040915. Biomedicines. 2024. PMID: 38672269 Free PMC article. Review.
-
Antiviral Activity and Crystal Structures of HIV-1 gp120 Antagonists.Int J Mol Sci. 2022 Dec 15;23(24):15999. doi: 10.3390/ijms232415999. Int J Mol Sci. 2022. PMID: 36555641 Free PMC article.
-
Week 96 Genotypic and Phenotypic Results of the Fostemsavir Phase 3 BRIGHTE Study in Heavily Treatment-Experienced Adults Living with Multidrug-Resistant HIV-1.Antimicrob Agents Chemother. 2022 Jun 21;66(6):e0175121. doi: 10.1128/aac.01751-21. Epub 2022 May 3. Antimicrob Agents Chemother. 2022. PMID: 35502922 Free PMC article. Clinical Trial.
References
-
- Ray N, Hwang C, Healy MD, et al. Prediction of virological response and assessment of resistance emergence to the HIV-1 attachment inhibitor BMS-626529 during 8-day monotherapy with its prodrug BMS-663068. J Acquir Immune Defic Syndr. 2013;64:7–15. - PubMed
-
- Zhou N, Nowicka-Sans B, McAuliffe B, et al. Genotypic correlates of susceptibility to HIV-1 attachment inhibitor BMS-626529, the active agent of the prodrug BMS-663068. J Antimicrob Chemother. 2014;69:573–581. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
