

Effects of women's groups practising participatory learning and action on preventive and care-seeking behaviours to reduce neonatal mortality: A meta-analysis of cluster-randomised trials
- PMID: 29206833
- PMCID: PMC5716527
- DOI: 10.1371/journal.pmed.1002467
Effects of women's groups practising participatory learning and action on preventive and care-seeking behaviours to reduce neonatal mortality: A meta-analysis of cluster-randomised trials
Abstract
Background: The World Health Organization recommends participatory learning and action (PLA) in women's groups to improve maternal and newborn health, particularly in rural settings with low access to health services. There have been calls to understand the pathways through which this community intervention may affect neonatal mortality. We examined the effect of women's groups on key antenatal, delivery, and postnatal behaviours in order to understand pathways to mortality reduction.
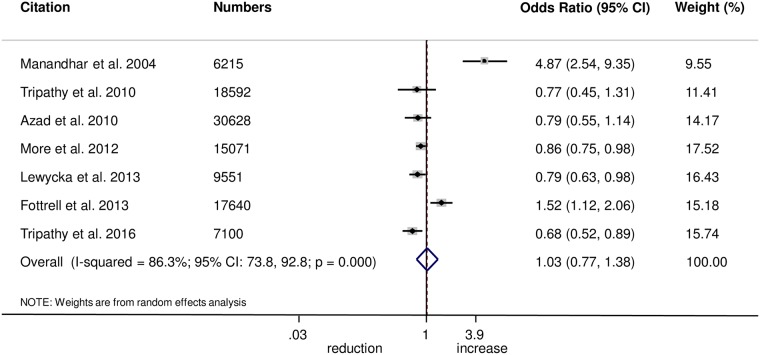
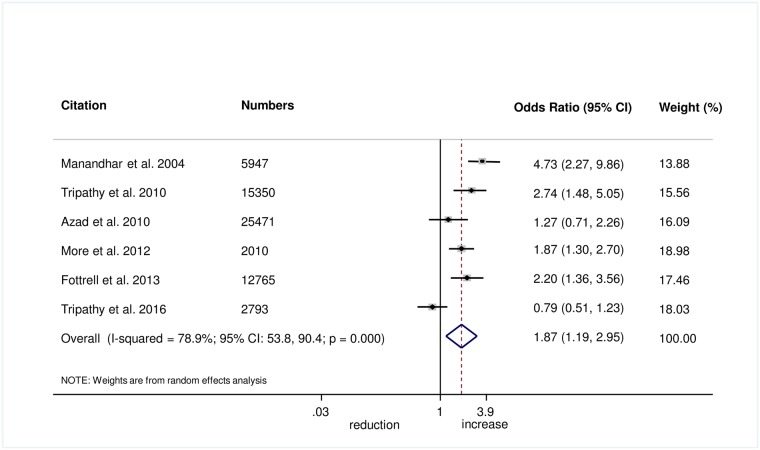
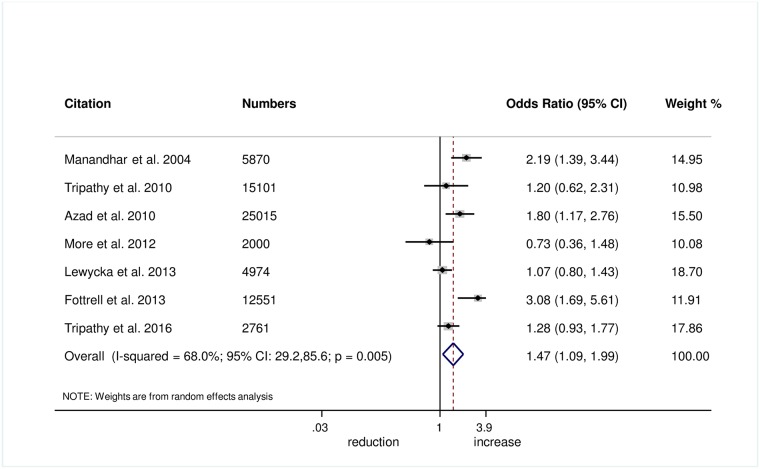
Methods and findings: We conducted a meta-analysis using data from 7 cluster-randomised controlled trials that took place between 2001 and 2012 in rural India (2 trials), urban India (1 trial), rural Bangladesh (2 trials), rural Nepal (1 trial), and rural Malawi (1 trial), with the number of participants ranging between 6,125 and 29,901 live births. Behavioural outcomes included appropriate antenatal care, facility delivery, use of a safe delivery kit, hand washing by the birth attendant prior to delivery, use of a sterilised instrument to cut the umbilical cord, immediate wrapping of the newborn after delivery, delayed bathing of the newborn, early initiation of breastfeeding, and exclusive breastfeeding. We used 2-stage meta-analysis techniques to estimate the effect of the women's group intervention on behavioural outcomes. In the first stage, we used random effects models with individual patient data to assess the effect of groups on outcomes separately for the different trials. In the second stage of the meta-analysis, random effects models were applied using summary-level estimates calculated in the first stage of the analysis. To determine whether behaviour change was related to group attendance, we used random effects models to assess associations between outcomes and the following categories of group attendance and allocation: women attending a group and allocated to the intervention arm; women not attending a group but allocated to the intervention arm; and women allocated to the control arm. Overall, women's groups practising PLA improved behaviours during and after home deliveries, including the use of safe delivery kits (odds ratio [OR] 2.92, 95% CI 2.02-4.22; I2 = 63.7%, 95% CI 4.4%-86.2%), use of a sterile blade to cut the umbilical cord (1.88, 1.25-2.82; 67.6%, 16.1%-87.5%), birth attendant washing hands prior to delivery (1.87, 1.19-2.95; 79%, 53.8%-90.4%), delayed bathing of the newborn for at least 24 hours (1.47, 1.09-1.99; 68.0%, 29.2%-85.6%), and wrapping the newborn within 10 minutes of delivery (1.27, 1.02-1.60; 0.0%, 0%-79.2%). Effects were partly dependent on the proportion of pregnant women attending groups. We did not find evidence of effects on uptake of antenatal care (OR 1.03, 95% CI 0.77-1.38; I2 = 86.3%, 95% CI 73.8%-92.8%), facility delivery (1.02, 0.93-1.12; 21.4%, 0%-65.8%), initiating breastfeeding within 1 hour (1.08, 0.85-1.39; 76.6%, 50.9%-88.8%), or exclusive breastfeeding for 6 weeks after delivery (1.18, 0.93-1.48; 72.9%, 37.8%-88.2%). The main limitation of our analysis is the high degree of heterogeneity for effects on most behaviours, possibly due to the limited number of trials involving women's groups and context-specific effects.
Conclusions: This meta-analysis suggests that women's groups practising PLA improve key behaviours on the pathway to neonatal mortality, with the strongest evidence for home care behaviours and practices during home deliveries. A lack of consistency in improved behaviours across all trials may reflect differences in local priorities, capabilities, and the responsiveness of health services. Future research could address the mechanisms behind how PLA improves survival, in order to adapt this method to improve maternal and newborn health in different contexts, as well as improve other outcomes across the continuum of care for women, children, and adolescents.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






Similar articles
-
The equity impact of community women's groups to reduce neonatal mortality: a meta-analysis of four cluster randomized trials.Int J Epidemiol. 2019 Feb 1;48(1):168-182. doi: 10.1093/ije/dyx160. Int J Epidemiol. 2019. PMID: 29024995 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Is essential newborn care provided by institutions and after home births? Analysis of prospective data from community trials in rural South Asia.BMC Pregnancy Childbirth. 2014 Mar 7;14:99. doi: 10.1186/1471-2393-14-99. BMC Pregnancy Childbirth. 2014. PMID: 24606612 Free PMC article. Clinical Trial.
-
Targeted client communication via mobile devices for improving maternal, neonatal, and child health.Cochrane Database Syst Rev. 2020 Jul 14;8(8):CD013679. doi: 10.1002/14651858.CD013679. Cochrane Database Syst Rev. 2020. PMID: 32813276 Free PMC article.
-
Effect of a participatory intervention with women's groups on birth outcomes in Nepal: cluster-randomised controlled trial.Lancet. 2004 Sep 11-17;364(9438):970-9. doi: 10.1016/S0140-6736(04)17021-9. Lancet. 2004. PMID: 15364188 Clinical Trial.
Cited by
-
Determinants of maternal low mid-upper arm circumference and its association with child nutritional status among poor and very poor households in rural Bangladesh.Matern Child Nutr. 2021 Oct;17(4):e13217. doi: 10.1111/mcn.13217. Epub 2021 May 20. Matern Child Nutr. 2021. PMID: 34018337 Free PMC article.
-
Intersectional role of paternal gender-equitable attitudes and maternal empowerment in child undernutrition: a cross-sectional national study from India.BMJ Open. 2021 Aug 5;11(8):e047276. doi: 10.1136/bmjopen-2020-047276. BMJ Open. 2021. PMID: 34353796 Free PMC article.
-
Health impact of self-help groups scaled-up statewide in Bihar, India.J Glob Health. 2020 Dec;10(2):021006. doi: 10.7189/jogh.10.021006. Epub 2020 Dec 19. J Glob Health. 2020. PMID: 33425330 Free PMC article.
-
Exploring the feasibility of a culturally tailored infant nutrition intervention: a qualitative study of perspectives from community facilitators and attendees in a pilot randomised controlled trial - Nurture Early for Optimal Nutrition (NEON) in East London.BMJ Public Health. 2024 Oct 31;2(2):e001358. doi: 10.1136/bmjph-2024-001358. eCollection 2024 Dec. BMJ Public Health. 2024. PMID: 40018531 Free PMC article.
-
Effectiveness of participatory women's groups scaled up by the public health system to improve birth outcomes in Jharkhand, eastern India: a pragmatic cluster non-randomised controlled trial.BMJ Glob Health. 2021 Nov;6(11):e005066. doi: 10.1136/bmjgh-2021-005066. BMJ Glob Health. 2021. PMID: 34732513 Free PMC article. Clinical Trial.
References
-
- Lawn J, Blencowe H, Oza S, You D, Lee ACC, Waiswa P, et al. Every Newborn: progress, priorities, and potential beyond survival. Lancet. 2014;384(9938):189–205. doi: 10.1016/S0140-6736(14)60496-7 - DOI - PubMed
-
- Lawn J, Cousens S, Zupan J. 4 million neonatal deaths: When? Where? Why? Lancet. 2005;365(9462):891–900. doi: 10.1016/S0140-6736(05)71048-5 - DOI - PubMed
-
- United Nations Children’s Fund, World Health Organization, World Bank Group, United Nations. Levels and trends in child mortality: report 2015. Estimates developed by the UN Inter-agency Group for Child Mortality Estimation. New York: United Nations Children’s Fund; 2015.
-
- Bhutta ZA, Das JK, Bahl R, Lawn JE, Salam RA, Paul VK, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. 2014;384(9940):347–70. doi: 10.1016/S0140-6736(14)60792-3 - DOI - PubMed
-
- Lassi Z, Haider B, Bhutta Z. Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Syst Rev. 2010;11:CD007754. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
