

Proportion and factors associated with recent HIV infection in a cohort of patients seen for care in Italy over 1996-2014: Data from the ICONA Foundation Study cohort
- PMID: 29206853
- PMCID: PMC5716540
- DOI: 10.1371/journal.pone.0189045
Proportion and factors associated with recent HIV infection in a cohort of patients seen for care in Italy over 1996-2014: Data from the ICONA Foundation Study cohort
Abstract
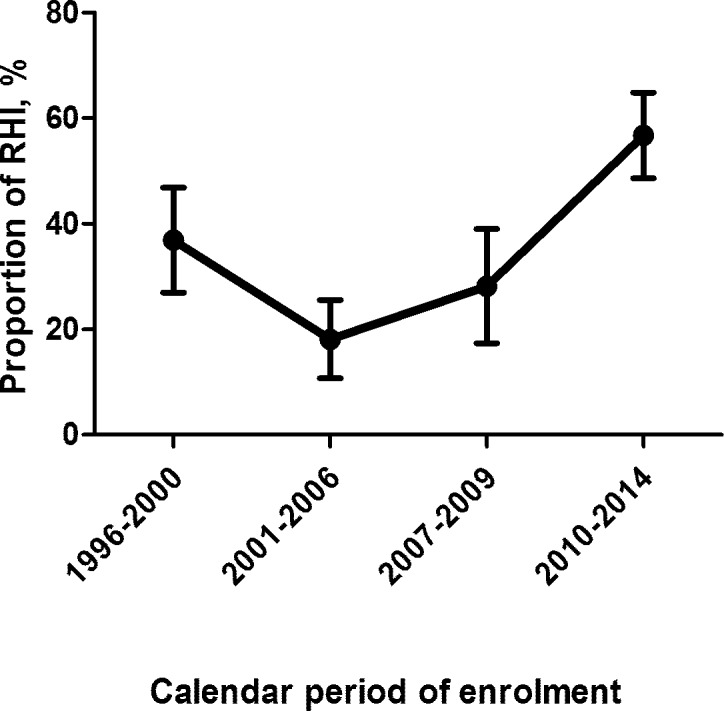
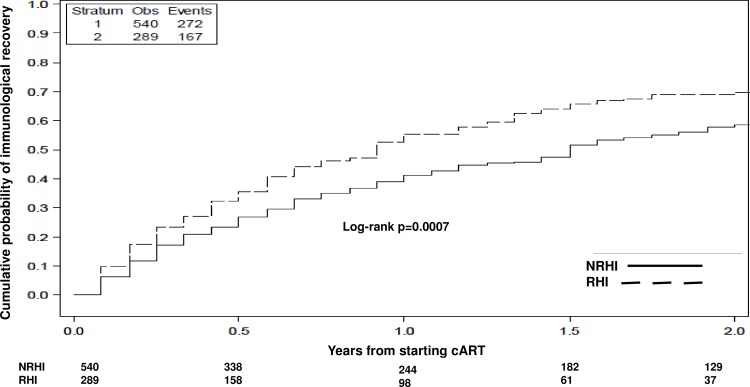
In Italy the prevalence of recent HIV infection (RHI) isn't currently monitored. Early diagnosis is crucial to allow introduction of antiretroviral therapy (cART) in the recent phase of infection. We aimed to estimate the proportion and the determinants of RHI among patients enrolled in the ICONA cohort; we explored differences in the median time from HIV diagnosis to cART initiation and in the viro-immunological response between RHI and Less Recent HIV infections (NRHI). We included antiretroviral-naïve HIV-positive patients enrolled in the cohort with documented dates of HIV-negative and positive antibodies tests, grouped in RHI (estimated date of seroconversion within 12 months of enrolment) and NRHI. Proportion of RHI and the trend of this proportion by calendar period (1996-2014) were investigated (Chi-square test). Logistic regression analysis was employed to identify factors associated with RHI. The time from seroconversion to cART initiation was compared in RHI and NRHI overall and after stratification by calendar period (survival analysis). We finally explored the time from starting cART to HIV-RNA <50 copies/mL and to CD4+ gain ≥200 cells/mmc by Cox regression. HIV seroconversion could be estimated for 2608/12,616 patients: 981/2608 (37.6%) were RHI. Proportion of RHI increased in recent calendar periods and was associated with younger age, baseline higher HIV-RNA and CD4+ count. There wasn't difference in the 2-year estimates of cART start between RHI and NRHI, regardless of calendar period. Rates and hazards of virological response were similar in RHI versus NRHI. RHI showed a 1.5-fold higher probability of CD4+ gain, also following adjustment for calendar period and cART regimen, and for age, HCV and smoking; the difference in probability was however attenuated after further controlling for baseline HIV-RNA and CD4+ T-cells. The increased proportion of RHI over time suggests that in recent years in Italy HIV infections are more likely to be detected earlier than before. The similar rates of cART introduction and viro-immunological response in RHI and NRHI probably reflect the efficacy of the modern cART regimens. An improvement of the prevention services is warranted to allow an early cART access, also in the perspective of therapy as prevention.
Conflict of interest statement
Figures
References
-
- Ryom L, Boesecke C, Gisler V, Manzardo C, Rockstroh JK, Puoti M, et al. Essentials from the 2015 European AIDS Clinical Society (EACS) guidelines for the treatment of adult HIV-positive persons. HIV Med. 2016;17(2):83–8. Epub 2015/11/08. doi: 10.1111/hiv.12322 . - DOI - PubMed
-
- Blaser N, Wettstein C, Estill J, Vizcaya LS, Wandeler G, Egger M, et al. Impact of viral load and the duration of primary infection on HIV transmission: systematic review and meta-analysis. AIDS. 2014;28(7):1021–9. doi: 10.1097/QAD.0000000000000135 ; PubMed Central PMCID: PMCPMC4058443. - DOI - PMC - PubMed
-
- Marzel A, Shilaih M, Yang WL, Böni J, Yerly S, Klimkait T, et al. HIV-1 Transmission During Recent Infection and During Treatment Interruptions as Major Drivers of New Infections in the Swiss HIV Cohort Study. Clin Infect Dis. 2016;62(1):115–22. Epub 2015/09/19. doi: 10.1093/cid/civ732 . - DOI - PubMed
-
- Mangal TD, EuroCoord UWGoCPaMAHSitCCi. Joint estimation of CD4+ cell progression and survival in untreated individuals with HIV-1 infection. AIDS. 2017;31(8):1073–82. doi: 10.1097/QAD.0000000000001437 ; PubMed Central PMCID: PMCPMC5414573. - DOI - PMC - PubMed
-
- Günthard HF, Saag MS, Benson CA, del Rio C, Eron JJ, Gallant JE, et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2016 Recommendations of the International Antiviral Society-USA Panel. JAMA. 2016;316(2):191–210. doi: 10.1001/jama.2016.8900 ; PubMed Central PMCID: PMCPMC5012643. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
