

Achieved systolic blood pressure in older people: a systematic review and meta-analysis
- PMID: 29207946
- PMCID: PMC5717809
- DOI: 10.1186/s12877-017-0672-4
Achieved systolic blood pressure in older people: a systematic review and meta-analysis
Abstract
Background: It remains unclear into which level the systolic blood pressure (SBP) should be lowered in order to provide the best cardiovascular protection among older people. Hypertension guidelines recommendation on attaining SBP levels <150 mmHg in this population is currently based on experts' opinion. To clarify this issue, we systematically reviewed and quantified available evidence on the impact of achieving different SBP levels <150 mmHg on various adverse outcomes in subjects aged ≥60 years old receiving antihypertensive drug treatment.
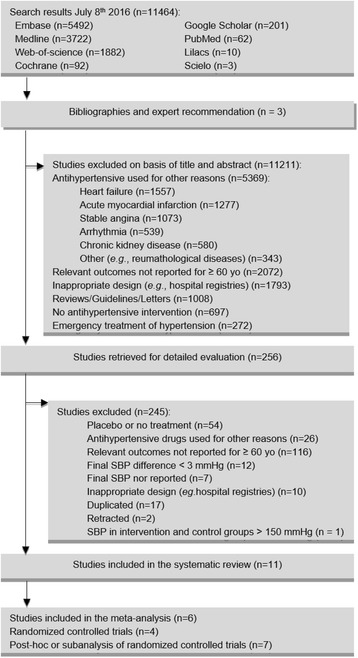
Methods: We searched 8 databases to identify randomized controlled trials (RCTs) and post-hoc analyses or subanalyses of RCTs reporting the effects of attaining different SBP levels <150 mmHg on the risk of stroke, acute myocardial infarction, heart failure, cardiovascular mortality and all-cause mortality in participants aged ≥60 years. We performed random-effects meta-analyses stratified by study design.
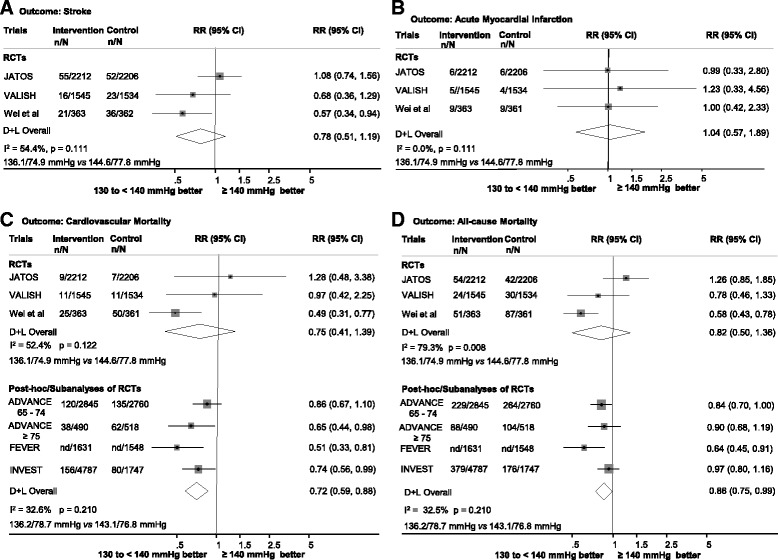
Results: Eleven studies (> 33,600 participants) were included. Compared with attaining SBP levels ≥140 mmHg, levels of 130 to <140 mmHg were not associated with lower risk of outcomes in the meta-analysis of RCTs, whereas there was an associated reduction of cardiovascular mortality (RR 0.72, 95% CI 0.59-0.88) and all-cause mortality (RR 0.86, 95% CI 0.75-0.99) in the meta-analysis of post-hoc analyses or subanalyses of RCTs. Limited and conflicting data were available for the SBP levels of <130 mmHg and 140 to <150 mmHg.
Conclusions: Among older people, there is suggestive evidence that achieving SBP levels of 130 to <140 mmHg is associated with lower risks of cardiovascular and all-cause mortality. Future trials are required to confirm these findings and to provide additional evidence regarding the <130 and 140 to <150 mmHg SBP levels.
Keywords: Aged; Antihypertensive agents; Antihypertensive drugs; Antihypertensives; Blood pressure; Hypertension; Older people.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable, since data for this systematic review and meta-analysis was collected from published studies.
Consent for publication
Not applicable, since data for this systematic review and meta-analysis was collected from published studies.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Pharmacotherapy for hypertension in adults aged 18 to 59 years.Cochrane Database Syst Rev. 2017 Aug 16;8(8):CD008276. doi: 10.1002/14651858.CD008276.pub2. Cochrane Database Syst Rev. 2017. PMID: 28813123 Free PMC article.
-
Blood pressure targets for the treatment of people with hypertension and cardiovascular disease.Cochrane Database Syst Rev. 2017 Oct 11;10(10):CD010315. doi: 10.1002/14651858.CD010315.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2018 Jul 20;7:CD010315. doi: 10.1002/14651858.CD010315.pub3. PMID: 29020435 Free PMC article. Updated.
-
Blood pressure targets for the treatment of people with hypertension and cardiovascular disease.Cochrane Database Syst Rev. 2018 Jul 20;7(7):CD010315. doi: 10.1002/14651858.CD010315.pub3. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Sep 9;9:CD010315. doi: 10.1002/14651858.CD010315.pub4. PMID: 30027631 Free PMC article. Updated.
-
Mobile phone-based interventions for improving adherence to medication prescribed for the primary prevention of cardiovascular disease in adults.Cochrane Database Syst Rev. 2018 Jun 22;6(6):CD012675. doi: 10.1002/14651858.CD012675.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 Mar 26;3:CD012675. doi: 10.1002/14651858.CD012675.pub3. PMID: 29932455 Free PMC article. Updated.
-
Blood pressure targets for the treatment of people with hypertension and cardiovascular disease.Cochrane Database Syst Rev. 2022 Nov 18;11(11):CD010315. doi: 10.1002/14651858.CD010315.pub5. Cochrane Database Syst Rev. 2022. PMID: 36398903 Free PMC article.
Cited by
-
Screening and treatment of hypertension in older adults: less is more?Public Health Rev. 2018 Sep 3;39:26. doi: 10.1186/s40985-018-0101-z. eCollection 2018. Public Health Rev. 2018. PMID: 30186660 Free PMC article. Review.
-
Continuity of Care and the Control of High Blood Pressure at Colombian Primary Care Services.Inquiry. 2021 Jan-Dec;58:469580211047043. doi: 10.1177/00469580211047043. Inquiry. 2021. PMID: 34620003 Free PMC article.
-
Novel Insight into the Serum Sphingolipid Fingerprint Characterizing Longevity.Int J Mol Sci. 2022 Feb 22;23(5):2428. doi: 10.3390/ijms23052428. Int J Mol Sci. 2022. PMID: 35269570 Free PMC article.
-
Hypertension management in older adults.F1000Res. 2020 Aug 19;9:F1000 Faculty Rev-1003. doi: 10.12688/f1000research.20323.1. eCollection 2020. F1000Res. 2020. PMID: 32850119 Free PMC article. Review.
-
Review on the management of cardiovascular risk factors in the elderly.J Geriatr Cardiol. 2022 Nov 28;19(11):894-927. doi: 10.11909/j.issn.1671-5411.2022.11.008. J Geriatr Cardiol. 2022. PMID: 36561061 Free PMC article.
References
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. - DOI - PMC - PubMed
-
- Aronow WS, Fleg JL, Pepine CJ, Artinian NT, Bakris G, Brown AS, et al. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation task force on clinical expert consensus documents. Circulation. 2011;123:2434–2506. doi: 10.1161/CIR.0b013e31821daaf6. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
