

Acute Zonal Occult Outer Retinopathy (AZOOR): a case report of vision improvement after intravitreal injection of Ozurdex
- PMID: 29207977
- PMCID: PMC5718015
- DOI: 10.1186/s12886-017-0638-5
Acute Zonal Occult Outer Retinopathy (AZOOR): a case report of vision improvement after intravitreal injection of Ozurdex
Abstract
Background: AZOOR was first described by Gass in 1993 as a syndrome with rapid loss of one or more extensive zones of the outer retinal segments. It is characterized by photopsia, minimal funduscopic changes, and electroretinographic abnormalities. The efficacy of systemic steroids in treating AZOOR has been previously described and advocated by the concept of autoimmune retinopathy. However, the use of intravitreal of sustained-released steroid had not been mentioned to date.
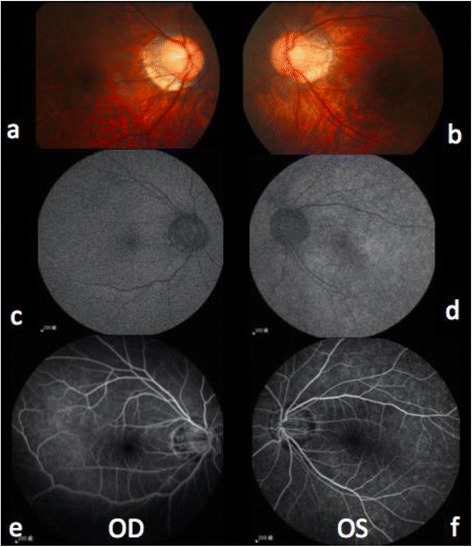
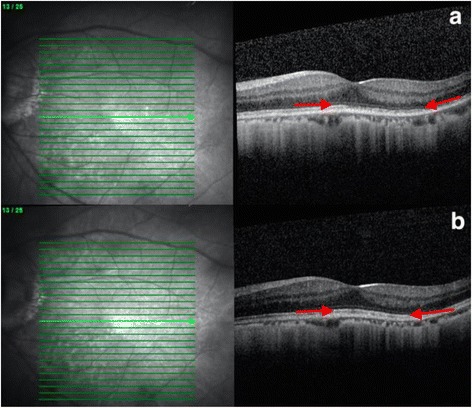
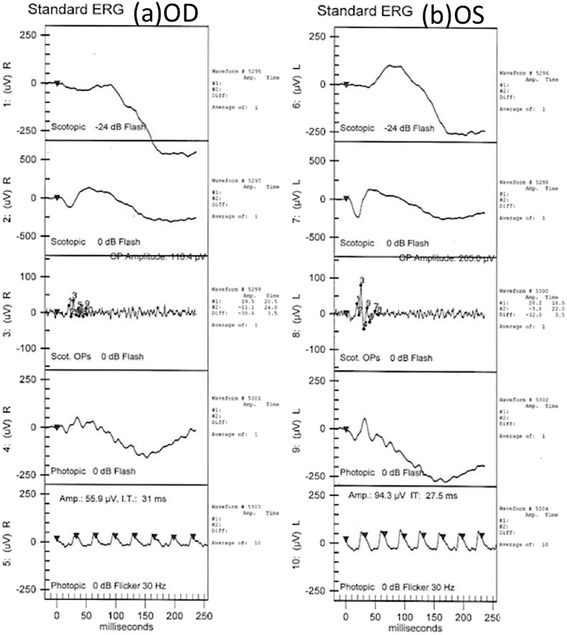
Case presentation: A 34-year-old man had sudden onset of central scotoma and photopsia in the left eye. His visual acuity continued deteriorating. The visual field defect demonstrated bilateral enlarged blind spots and altitudinal defects. Fluorescein angiography (FA) showed nonspecific retinal inflammation, and an electroretinogram (ERG) illustrated decreased amplitude of the b wave in both eyes. Optical coherence tomography (OCT) examinations revealed parafoveal loss of the photoreceptor inner/outer segment (IS/OS) junction. Therefore, acute zonal occult outer retinopathy (AZOOR) was diagnosed. Although his vision did not improve under the initial treatment of systemic corticosteroid and calcium channel blocker, remarkable improvement was noticed after the intravitreal injection(IVI) of Ozurdex, consistent with the recovered IS/OS junction disruption.
Conclusions: We herein report a typical case of AZOOR, suggesting that the intravitreal injection of steroid may benefit in certain patients.
Keywords: Acute zonal occult outer retinopathy; Electroretinogram; Optical coherence tomography; Sustained-released steroid.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Our patient consent to publish the image of eyes and other results of his medical examination in this manuscript or paper which may be published in your journal. Written consent was obtained from our patient.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Gass JD. Acute zonal occult outer retinopathy. Donders lecture: The Netherlands ophthalmological society, Maastricht, Holland, June 19, 1992. J Clin Neuroophthalmol. 1993;13(2):79–97. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
