

Estimating the likely true changes in rheumatic fever incidence using two data sources
- PMID: 29208066
- PMCID: PMC9134743
- DOI: 10.1017/S0950268817002734
Estimating the likely true changes in rheumatic fever incidence using two data sources
Abstract
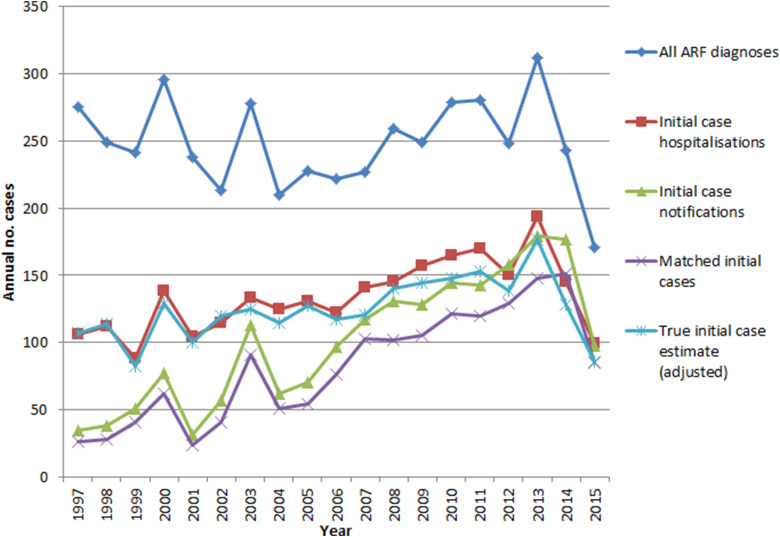
Acute rheumatic fever (ARF) continues to produce a significant burden of disease in New Zealand (NZ) Māori and Pacific peoples. Serious limitations in national surveillance data mean that accurate case totals cannot be generated. Given the changing epidemiology of ARF in NZ and the major national rheumatic fever prevention programme (2012-2017), we updated our previous likely true case number estimates using capture-recapture analyses. Aims were to estimate the likely true incidence of ARF in NZ and comment on the changing ability to detect cases. Data were obtained from national hospitalisation and notification databases. The Chapman Estimate partially adjusted for bias. An estimated 2342 likely true new cases arose from 1997 to 2015, giving a mean annual incidence of 2·9 per 100 000 (95% CI 2·5-3·5). Compared with the pre-intervention (2009-2011) baseline incidence (3·4 per 100 000, 95% CI 2·9-4·0), the likely true 2015 incidence declined 44%. Large gaps in data completeness are slowly closing. During the period 2012-2015, 723 cases were identified; 83·8% of notifications were matched to hospitalisation data, and 87·2% of hospitalisations matched to notifications. Despite this improvement, clinicians need to remain aware of the need to notify atypical patients. A possible unintended consequence of the national ARF prevention programme is increased misdiagnosis.
Keywords: Health equity; incidence; public health; rheumatic fever; surveillance system.
Conflict of interest statement
None.
Figures


Similar articles
-
Estimating rheumatic fever incidence in New Zealand using multiple data sources.Epidemiol Infect. 2015 Jan;143(1):167-77. doi: 10.1017/S0950268814000296. Epub 2014 Mar 6. Epidemiol Infect. 2015. PMID: 24598156 Free PMC article.
-
Epidemiology of acute rheumatic fever in New Zealand 1996-2005.J Paediatr Child Health. 2008 Oct;44(10):564-71. doi: 10.1111/j.1440-1754.2008.01384.x. J Paediatr Child Health. 2008. PMID: 19012628
-
The epidemiology of acute rheumatic fever in Northland, 2012-2017.N Z Med J. 2019 Jul 12;132(1498):32-40. N Z Med J. 2019. PMID: 31295236
-
Risk Factors for Acute Rheumatic Fever: Literature Review and Protocol for a Case-Control Study in New Zealand.Int J Environ Res Public Health. 2019 Nov 15;16(22):4515. doi: 10.3390/ijerph16224515. Int J Environ Res Public Health. 2019. PMID: 31731673 Free PMC article. Review.
-
Comparison of approaches to rheumatic fever surveillance across Organisation for Economic Co-operation and Development countries.J Paediatr Child Health. 2015 Nov;51(11):1071-7. doi: 10.1111/jpc.12969. Epub 2015 Jul 14. J Paediatr Child Health. 2015. PMID: 26174709 Review.
Cited by
-
Acute rheumatic fever and rheumatic heart disease in children and adolescents in Victoria, Australia.J Paediatr Child Health. 2023 Feb;59(2):352-359. doi: 10.1111/jpc.16305. Epub 2022 Dec 8. J Paediatr Child Health. 2023. PMID: 36478625 Free PMC article.
-
Acute rheumatic fever and rheumatic heart disease in Victoria, 2006-18.Med J Aust. 2022 Mar 7;216(4):201-202. doi: 10.5694/mja2.51374. Epub 2021 Dec 27. Med J Aust. 2022. PMID: 34961922 Free PMC article. No abstract available.
-
Ethnically Disparate Disease Progression and Outcomes among Acute Rheumatic Fever Patients in New Zealand, 1989-2015.Emerg Infect Dis. 2021 Jul;27(7):1893-902. doi: 10.3201/eid2707.203045. Emerg Infect Dis. 2021. PMID: 34153221 Free PMC article.
-
Preceding group A streptococcus skin and throat infections are individually associated with acute rheumatic fever: evidence from New Zealand.BMJ Glob Health. 2021 Dec;6(12):e007038. doi: 10.1136/bmjgh-2021-007038. BMJ Glob Health. 2021. PMID: 34887304 Free PMC article.
-
C10Pred: A First Machine Learning Based Tool to Predict C10 Family Cysteine Peptidases Using Sequence-Derived Features.Int J Mol Sci. 2022 Aug 23;23(17):9518. doi: 10.3390/ijms23179518. Int J Mol Sci. 2022. PMID: 36076915 Free PMC article.
References
-
- Milne RJ, et al. Incidence of acute rheumatic fever in New Zealand children and youth. Journal of Paediatrics & Child Health 2012; 48(8): 685–691. - PubMed
-
- Jack S, et al. Interim Evaluation of the Sore Throat Component of the Rheumatic Fever Prevention Programme – Quantitative Findings. Porirua, New Zealand: The Institute of Environmental Science and Research Ltd, 2015. (https://www.health.govt.nz/system/files/documents/publications/interim-e...).
-
- Carapetis JR, et al. The global burden of group A streptococcal diseases. The Lancet Infectious Diseases 2005; 5(11): 685–694. - PubMed
-
- Vendsborg P, Hansen LF, Olesen KH. Decreasing incidence of a history of acute rheumatic fever in chronic rheumatic heart disease. Cardiologia 1968; 53(6): 332–340. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
