

Short-term clinical outcomes of laparoscopic vs open rectal excision for rectal cancer: A systematic review and meta-analysis
- PMID: 29209132
- PMCID: PMC5703920
- DOI: 10.3748/wjg.v23.i44.7906
Short-term clinical outcomes of laparoscopic vs open rectal excision for rectal cancer: A systematic review and meta-analysis
Abstract
Aim: To review evidence on the short-term clinical outcomes of laparoscopic (LRR) vs open rectal resection (ORR) for rectal cancer.
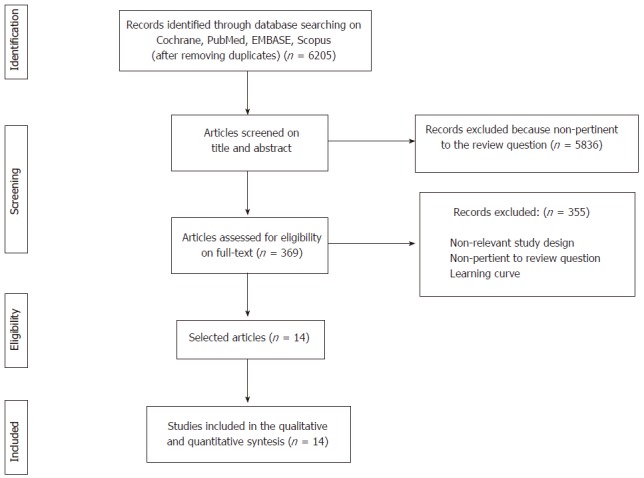
Methods: A systematic literature search was performed using Cochrane Central Register, MEDLINE, EMBASE, Scopus, OpenGrey and ClinicalTrials.gov register for randomized clinical trials (RCTs) comparing LRR vs ORR for rectal cancer and reporting short-term clinical outcomes. Articles published in English from January 1, 1995 to June, 30 2016 that met the selection criteria were retrieved and reviewed. The Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) statements checklist for reporting a systematic review was followed. Random-effect models were used to estimate mean differences and risk ratios. The robustness and heterogeneity of the results were explored by performing sensitivity analyses. The pooled effect was considered significant when P < 0.05.
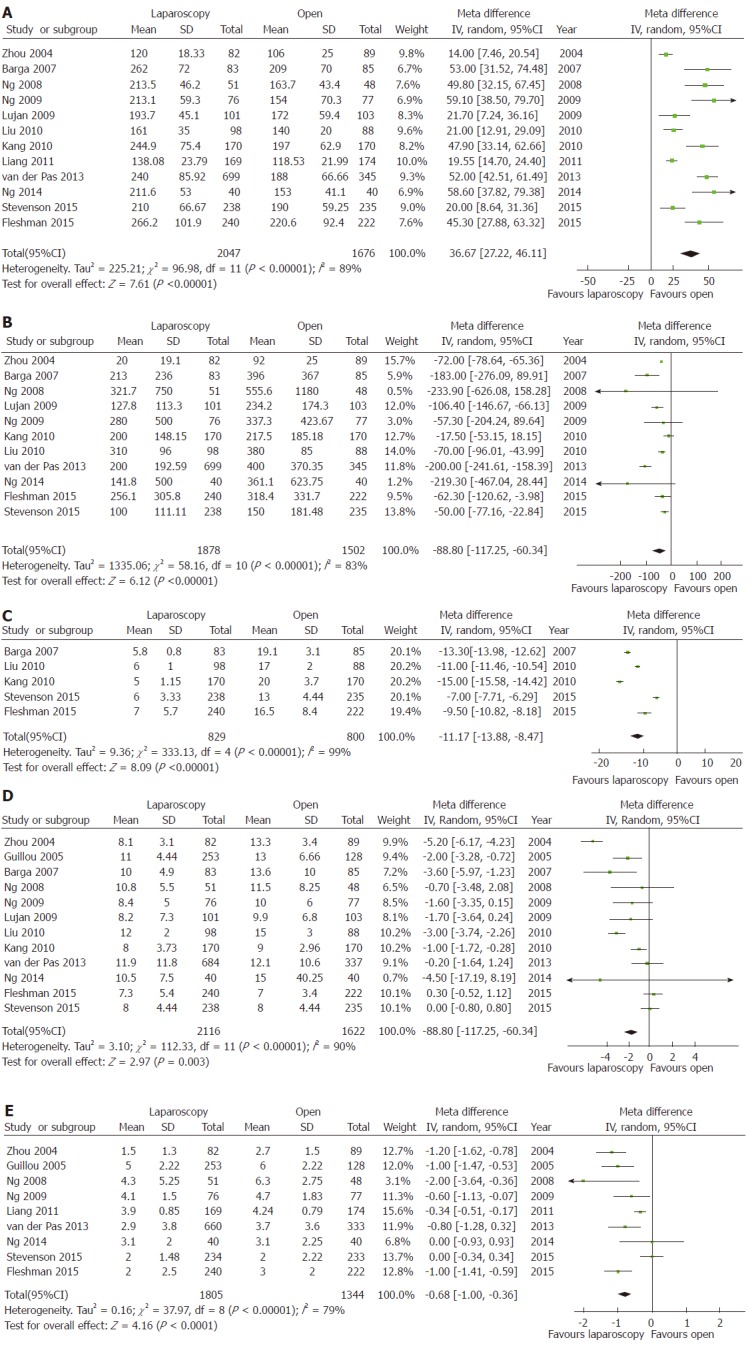
Results: Overall, 14 RCTs were included. No differences were found in postoperative mortality (P = 0.19) and morbidity (P = 0.75) rates. The mean operative time was 36.67 min longer (95%CI: 27.22-46.11, P < 0.00001), the mean estimated blood loss was 88.80 ml lower (95%CI: -117.25 to -60.34, P < 0.00001), and the mean incision length was 11.17 cm smaller (95%CI: -13.88 to -8.47, P < 0.00001) for LRR than ORR. These results were confirmed by sensitivity analyses that focused on the four major RCTs. The mean length of hospital stay was 1.71 d shorter (95%CI: -2.84 to -0.58, P < 0.003) for LRR than ORR. Similarly, bowel recovery (i.e., day of the first bowel movement) was 0.68 d shorter (95%CI: -1.00 to -0.36, P < 0.00001) for LRR. The sensitivity analysis did not confirm a significant difference between LRR and ORR for these latter two parameters. The overall quality of the evidence was rated as high.
Conclusion: LRR is associated with lesser blood loss, smaller incision length, and longer operative times compared to ORR. No differences are observed for postoperative morbidity and mortality.
Keywords: Laparoscopic rectal resection; Laparoscopy; Meta-analysis; Open rectal resection; Postoperative morbidity; Rectal cancer; Short-term outcomes; Systematic review.
Conflict of interest statement
Conflict-of-interest statement: The authors deny any conflict of interest.
Figures
Similar articles
-
Pathologic Outcomes of Laparoscopic vs Open Mesorectal Excision for Rectal Cancer: A Systematic Review and Meta-analysis.JAMA Surg. 2017 Apr 19;152(4):e165665. doi: 10.1001/jamasurg.2016.5665. Epub 2017 Apr 19. JAMA Surg. 2017. PMID: 28196217
-
Laparoscopic versus open resection for sigmoid diverticulitis.Cochrane Database Syst Rev. 2017 Nov 25;11(11):CD009277. doi: 10.1002/14651858.CD009277.pub2. Cochrane Database Syst Rev. 2017. PMID: 29178125 Free PMC article.
-
Robotic resection compared with laparoscopic rectal resection for cancer: systematic review and meta-analysis of short-term outcome.Colorectal Dis. 2012 Apr;14(4):e134-56. doi: 10.1111/j.1463-1318.2011.02907.x. Colorectal Dis. 2012. PMID: 22151033
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.Health Technol Assess. 2006 Nov;10(45):1-141, iii-iv. doi: 10.3310/hta10450. Health Technol Assess. 2006. PMID: 17083853
-
Transanal total mesorectal excision (taTME) for rectal cancer: a systematic review and meta-analysis of oncological and perioperative outcomes compared with laparoscopic total mesorectal excision.BMC Cancer. 2016 Jul 4;16:380. doi: 10.1186/s12885-016-2428-5. BMC Cancer. 2016. PMID: 27377924 Free PMC article.
Cited by
-
Clinical and oncological outcomes of the low ligation of the inferior mesenteric artery with robotic surgery in patients with rectal cancer following neoadjuvant chemoradiotherapy.Turk J Med Sci. 2021 Feb 26;51(1):111-123. doi: 10.3906/sag-2003-178. Turk J Med Sci. 2021. PMID: 32777903 Free PMC article.
-
Comparative analysis of the safety and effectiveness of robotic natural orifice specimen extraction versus laparoscopic surgery for colorectal tumors through systematic review and meta-analysis.J Robot Surg. 2024 Oct 19;18(1):374. doi: 10.1007/s11701-024-02090-7. J Robot Surg. 2024. PMID: 39427105 Free PMC article.
-
Open versus minimally invasive surgery for rectal cancer: a single-center cohort study on 237 consecutive patients.Updates Surg. 2019 Sep;71(3):493-504. doi: 10.1007/s13304-019-00642-3. Epub 2019 Mar 13. Updates Surg. 2019. PMID: 30868546
-
Mid- and low-rectal cancer: laparoscopic vs open treatment-short- and long-term results. Meta-analysis of randomized controlled trials.Int J Colorectal Dis. 2022 Jan;37(1):71-99. doi: 10.1007/s00384-021-04048-9. Epub 2021 Oct 29. Int J Colorectal Dis. 2022. PMID: 34716474
-
Impact of Low- Versus Standard-Pressure Pneumoperitoneum on Postoperative Recovery in Patients with Obesity Undergoing Robot-Assisted Radical Prostatectomy: A Retrospective Cohort Study.Medicina (Kaunas). 2025 Jul 10;61(7):1253. doi: 10.3390/medicina61071253. Medicina (Kaunas). 2025. PMID: 40731882 Free PMC article.
References
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1:1479–1482. - PubMed
-
- Lee M, Gibbs P, Wong R. Multidisciplinary Management of Locally Advanced Rectal Cancer--An Evolving Landscape? Clin Colorectal Cancer. 2015;14:251–261. - PubMed
-
- van der Pas MH, Haglind E, Cuesta MA, Fürst A, Lacy AM, Hop WC, Bonjer HJ; COlorectal cancer Laparoscopic or Open Resection II (COLOR II) Study Group. Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 2013;14:210–218. - PubMed
-
- Kang SB, Park JW, Jeong SY, Nam BH, Choi HS, Kim DW, Lim SB, Lee TG, Kim DY, Kim JS, et al. Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): short-term outcomes of an open-label randomised controlled trial. Lancet Oncol. 2010;11:637–645. - PubMed
-
- Fleshman J, Branda M, Sargent DJ, Boller AM, George V, Abbas M, Peters WR Jr, Maun D, Chang G, Herline A, Fichera A, Mutch M, Wexner S, Whiteford M, Marks J, Birnbaum E, Margolin D, Larson D, Marcello P, Posner M, Read T, Monson J, Wren SM, Pisters PW, Nelson H. Effect of Laparoscopic-Assisted Resection vs Open Resection of Stage II or III Rectal Cancer on Pathologic Outcomes: The ACOSOG Z6051 Randomized Clinical Trial. JAMA. 2015;314:1346–1355. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
