

If Time Is Brain Where Is the Improvement in Prehospital Time after Stroke?
- PMID: 29209269
- PMCID: PMC5701972
- DOI: 10.3389/fneur.2017.00617
If Time Is Brain Where Is the Improvement in Prehospital Time after Stroke?
Abstract
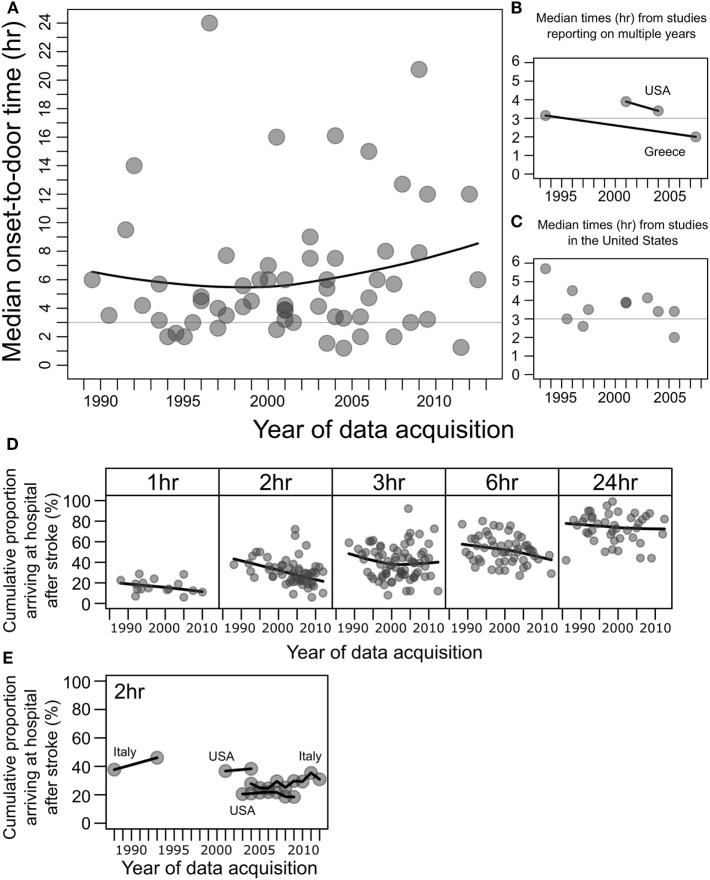
Despite the availability of thrombolytic and endovascular therapy for acute ischemic stroke, many patients are ineligible due to delayed hospital arrival. The identification of factors related to either early or delayed hospital arrival may reveal potential targets of intervention to reduce prehospital delay and improve access to time-critical thrombolysis and clot retrieval therapy. Here, we have reviewed studies reporting on factors associated with either early or delayed hospital arrival after stroke, together with an analysis of stroke onset to hospital arrival times. Much effort in the stroke treatment community has been devoted to reducing door-to-needle times with encouraging improvements. However, this review has revealed that the median onset-to-door times and the percentage of stroke patients arriving before the logistically critical 3 h have shown little improvement in the past two decades. Major factors affecting prehospital time were related to emergency medical pathways, stroke symptomatology, patient and bystander behavior, patient health characteristics, and stroke treatment awareness. Interventions addressing these factors may prove effective in reducing prehospital delay, allowing prompt diagnosis, which in turn may increase the rates and/or efficacy of acute treatments such as thrombolysis and clot retrieval therapy and thereby improve stroke outcomes.
Keywords: emergency medical services; prehospital delay; stroke; thrombolysis; tissue plasminogen activator.
Figures
References
-
- Hacke W, Kaste M, Fieschi C, Von Kummer R, Davalos A, Meier D, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet (1998) 352:1245–51.10.1016/S0140-6736(98)08020-9 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous