

Meckel-Gruber Syndrome: An Update on Diagnosis, Clinical Management, and Research Advances
- PMID: 29209597
- PMCID: PMC5701918
- DOI: 10.3389/fped.2017.00244
Meckel-Gruber Syndrome: An Update on Diagnosis, Clinical Management, and Research Advances
Abstract
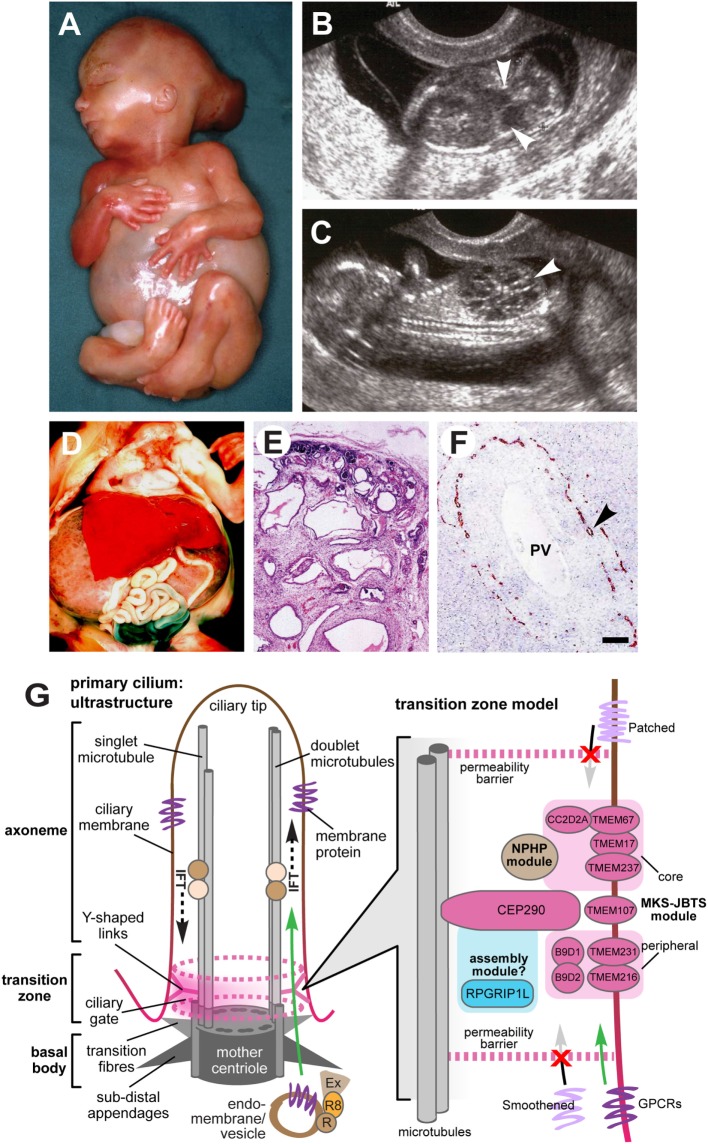
Meckel-Gruber syndrome (MKS) is a lethal autosomal recessive congenital anomaly syndrome caused by mutations in genes encoding proteins that are structural or functional components of the primary cilium. Conditions that are caused by mutations in ciliary genes are collectively termed the ciliopathies, and MKS represents the most severe condition in this group of disorders. The primary cilium is a microtubule-based organelle, projecting from the apical surface of vertebrate cells. It acts as an "antenna" that receives and transduces chemosensory and mechanosensory signals, but also regulates diverse signaling pathways, such as Wnt and Shh, that have important roles during embryonic development. Most MKS proteins localize to a distinct ciliary compartment called the transition zone (TZ) that regulates the trafficking of cargo proteins or lipids. In this review, we provide an up-to-date summary of MKS clinical features, molecular genetics, and clinical diagnosis. MKS has a highly variable phenotype, extreme genetic heterogeneity, and displays allelism with other related ciliopathies such as Joubert syndrome, presenting significant challenges to diagnosis. Recent advances in genetic technology, with the widespread use of multi-gene panels for molecular testing, have significantly improved diagnosis, genetic counseling, and the clinical management of MKS families. These include the description of some limited genotype-phenotype correlations. We discuss recent insights into the molecular basis of disease in MKS, since the functions of some of the relevant ciliary proteins have now been determined. A common molecular etiology appears to be disruption of ciliary TZ structure and function, affecting essential developmental signaling and the regulation of secondary messengers.
Keywords: Meckel–Gruber syndrome; Shh signaling; oligohydramnios; primary cilium; renal cystic dysplasia; transition zone.
Figures
References
-
- Meckel J. Beschreibung zweier, durch sehr ähnliche Bildungsabweichungen entstellter Geschwister. Dtsch Arch Physiol (1882) 7:99–172.
-
- Gruber G. Beitrage zur frage “gekoppelter” Miszbildungen (Akrocephalo-syndactylie und dysencephalia splanchnocystica). Beitr Pathol Anat (1934) 93:459–76.
-
- Opitz JM, Howe JJ. The Meckel syndrome (dysencephalia splanchnocystica, the Grüber syndrome). Birth Defects Orig Art Ser (1969) 2:167–79.
-
- Mecke S, Passarge E. Encephalocele, polycystic kidneys and polydactyly as an autosomal recessive trait simulating certain other disorders – Meckel syndrome. Ann Genet (1971) 14:97–103. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources