

Effect of High-Cutoff Hemodialysis vs Conventional Hemodialysis on Hemodialysis Independence Among Patients With Myeloma Cast Nephropathy: A Randomized Clinical Trial
- PMID: 29209721
- PMCID: PMC5820717
- DOI: 10.1001/jama.2017.17924
Effect of High-Cutoff Hemodialysis vs Conventional Hemodialysis on Hemodialysis Independence Among Patients With Myeloma Cast Nephropathy: A Randomized Clinical Trial
Abstract
Importance: Cast nephropathy is the main cause of acute kidney injury in multiple myeloma and persistent reduction in kidney function strongly affects prognosis. Strategies to rapidly remove nephrotoxic serum-free light chains combined with novel antimyeloma agents have not been evaluated prospectively.
Objective: To compare the hemodialysis independence rate among patients newly diagnosed with myeloma cast nephropathy treated with hemodialysis using a high-cutoff dialyzer (with very large membrane pores and high permeability to immunoglobulin light chains) or a conventional high-flux dialyzer (with small pores and lower permeability).
Design, setting, and participants: Randomized clinical trial involving 98 patients with biopsy-proven myeloma cast nephropathy requiring hemodialysis treated at 48 French centers between July 2011 and June 2016; the final date of follow-up was June 29, 2016.
Interventions: Intensive hemodialysis (eight 5-hour sessions over 10 days) with either a high-cutoff dialyzer (46 patients) or a conventional high-flux dialyzer (48 patients). All patients received the same chemotherapy regimen of bortezomib and dexamethasone.
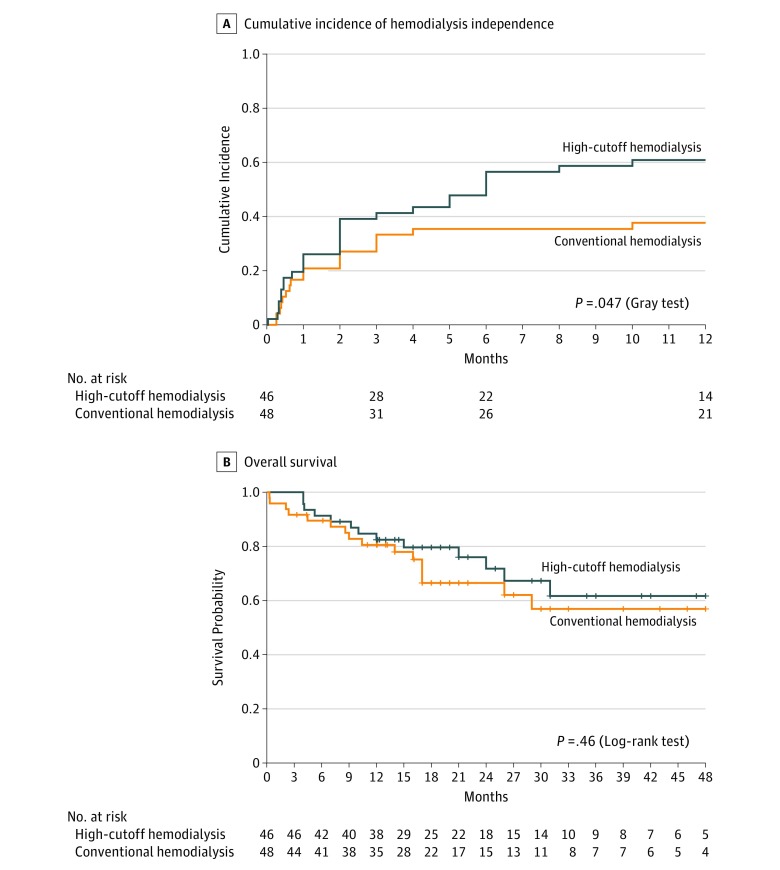
Main outcomes and measures: Primary end point was hemodialysis independence at 3 months; secondary end points: hemodialysis independence rates at 6 and 12 months, hemodialysis- and chemotherapy-related adverse events, and death.
Results: Among 98 randomized patients, 94 (96%) (median age, 68.8 years [interquartile range, 61.2-75.3 years]; 45% women) were included in the modified intent-to-treat analysis. The hemodialysis independence rate at 3 months was 41.3% (n = 19) in the high-cutoff hemodialysis group vs 33.3% (n = 16) in the conventional hemodialysis group (between-group difference, 8.0% [95% CI, -12.0% to 27.9%], P = .42); at 6 months, the rate was 56.5% (n = 26) vs 35.4% (n = 17), respectively (between-group difference, 21.1% [95% CI, 0.9% to 41.3%], P = .04); and at 12 months, the rate was 60.9% (n = 28) vs 37.5% (n = 18) (between-group difference, 23.4% [95% CI, 3.2% to 43.5%], P = .02). The incidence of hemodialysis-related adverse events was 43% in the high-cutoff hemodialysis group vs 39% in the conventional hemodialysis group; chemotherapy-related serious adverse events, 39% vs 37%, respectively; and at 12 months, 9 patients vs 10 patients died.
Conclusions and relevance: Among patients with myeloma cast nephropathy treated with a bortezomib-based chemotherapy regimen, the use of high-cutoff hemodialysis compared with conventional hemodialysis did not result in a statistically significant difference in hemodialysis independence at 3 months. However, the study may have been underpowered to identify an early clinically important difference.
Trial registration: clinicaltrials.gov Identifier: NCT01208818.
Conflict of interest statement
Figures

Comment in
-
High-Cutoff Hemodialysis in Myeloma Cast Nephropathy.JAMA. 2017 Dec 5;318(21):2085-2086. doi: 10.1001/jama.2017.18710. JAMA. 2017. PMID: 29209704 No abstract available.
References
-
- Dimopoulos MA, Sonneveld P, Leung N, et al. . International Myeloma Working Group recommendations for the diagnosis and management of myeloma-related renal impairment. J Clin Oncol. 2016;34(13):1544-1557. - PubMed
-
- Yadav P, Hutchison CA, Basnayake K, et al. . Patients with multiple myeloma have excellent long-term outcomes after recovery from dialysis-dependent acute kidney injury. Eur J Haematol. 2016;96(6):610-617. - PubMed
-
- Clark WF, Stewart AK, Rock GA, et al. . Plasma exchange when myeloma presents as acute renal failure. Ann Intern Med. 2005;143(11):777-784. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
