

The effects of the attributable fraction and the duration of symptoms on burden estimates of influenza-associated respiratory illnesses in a high HIV prevalence setting, South Africa, 2013-2015
- PMID: 29210203
- PMCID: PMC5907815
- DOI: 10.1111/irv.12529
The effects of the attributable fraction and the duration of symptoms on burden estimates of influenza-associated respiratory illnesses in a high HIV prevalence setting, South Africa, 2013-2015
Abstract
Background: The attributable fraction of influenza virus detection to illness (INF-AF) and the duration of symptoms as a surveillance inclusion criterion could potentially have substantial effects on influenza disease burden estimates.
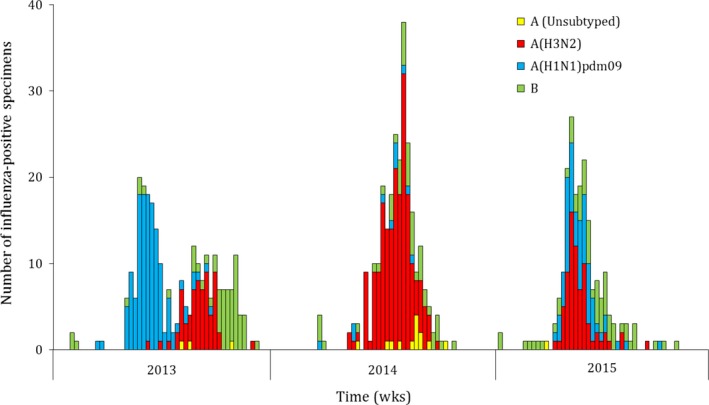
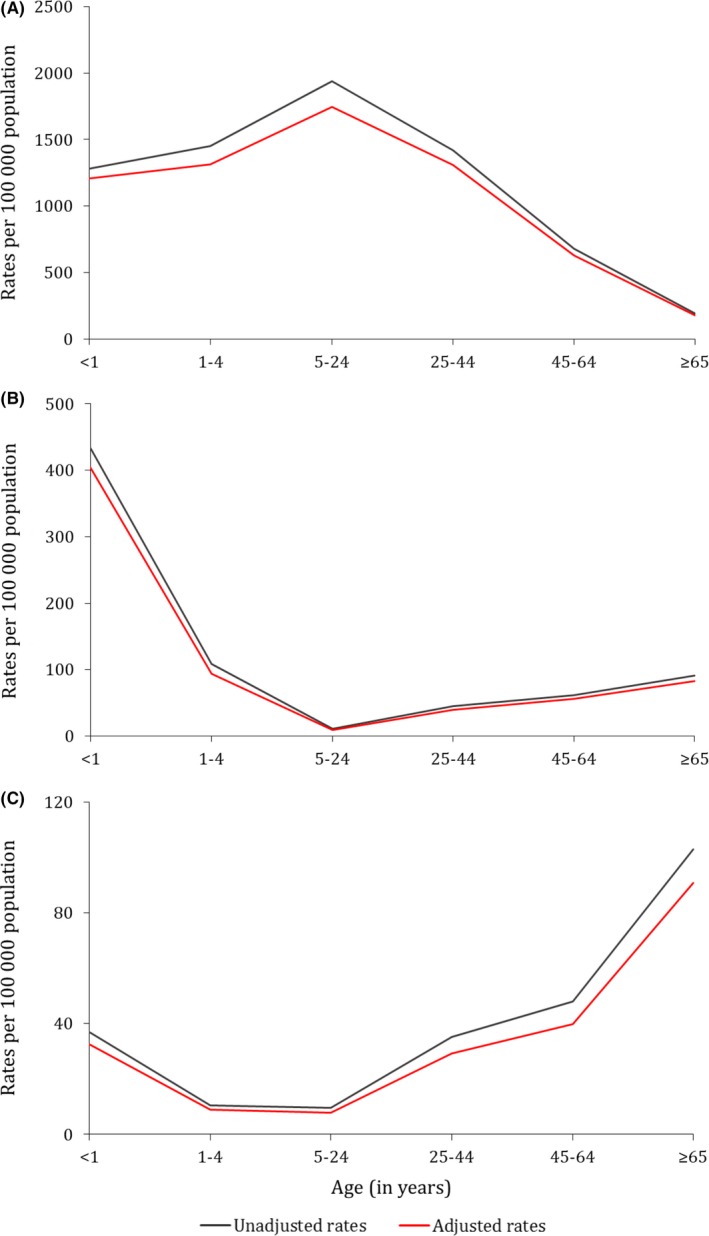
Methods: We estimated rates of influenza-associated influenza-like illness (ILI) and severe acute (SARI-10) or chronic (SCRI-10) respiratory illness (using a symptom duration cutoff of ≤10 days) among HIV-infected and HIV-uninfected patients attending 3 hospitals and 2 affiliated clinics in South Africa during 2013-2015. We calculated the unadjusted and INF-AF-adjusted rates and relative risk (RR) due to HIV infection. Rates were expressed per 100 000 population.
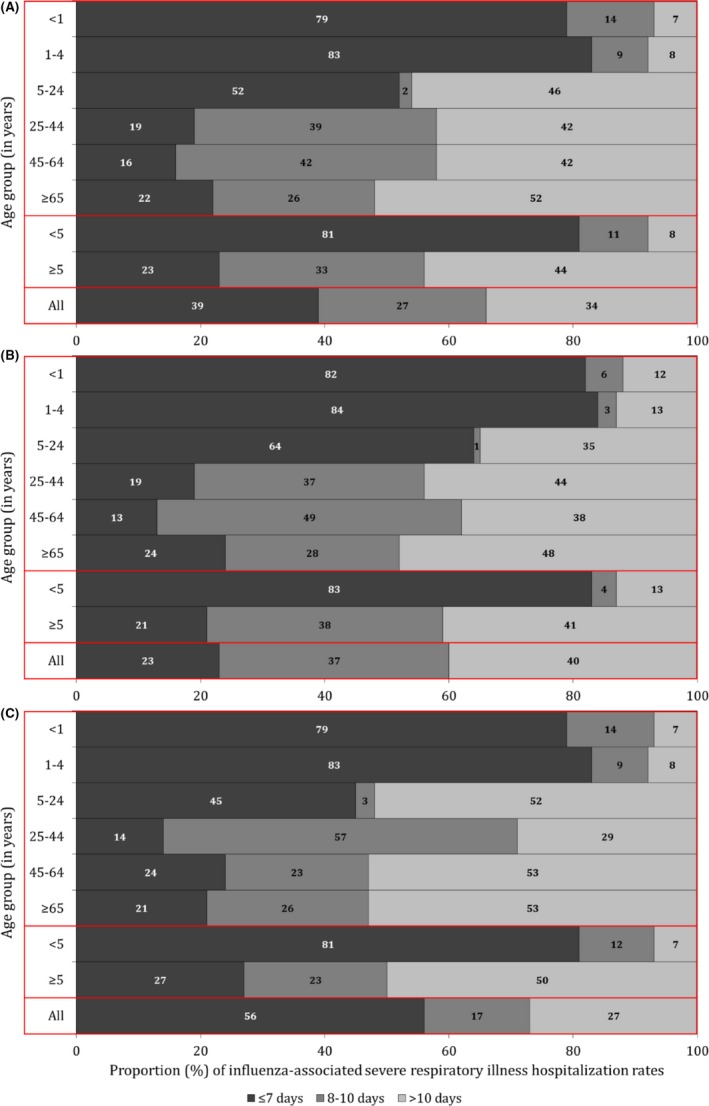
Results: The estimated mean annual unadjusted rates of influenza-associated illness were 1467.7, 50.3, and 27.4 among patients with ILI, SARI-10, and SCRI-10, respectively. After adjusting for the INF-AF, the percent reduction in the estimated rates was 8.9% (rate: 1336.9), 11.0% (rate: 44.8), and 16.3% (rate: 22.9) among patients with ILI, SARI-10, and SCRI-10, respectively. HIV-infected compared to HIV-uninfected individuals experienced a 2.3 (95% CI: 2.2-2.4)-, 9.7 (95% CI: 8.0-11.8)-, and 10.0 (95% CI: 7.9-12.7)-fold increased risk of influenza-associated illness among patients with ILI, SARI-10, and SCRI-10, respectively. Overall 34% of the estimated influenza-associated hospitalizations had symptom duration of >10 days; 8% and 44% among individuals aged <5 and ≥5 years, respectively.
Conclusion: The marginal differences between unadjusted and INF-AF-adjusted rates are unlikely to affect policies on prioritization of interventions. HIV-infected individuals experienced an increased risk of influenza-associated illness and may benefit more from annual influenza immunization. The use of a symptom duration cutoff of ≤10 days may underestimate influenza-associated disease burden, especially in older individuals.
Keywords: HIV; South Africa; attributable fraction; influenza; influenza-like illness; rates; severe respiratory illness; symptom duration.
© 2017 The Authors. Influenza and Other Respiratory Viruses Published by John Wiley & Sons Ltd.
Figures
References
-
- Simonsen L, Clarke MJ, Schonberger LB, et al. Pandemic versus epidemic influenza mortality: a pattern of changing age distribution. J Infect Dis. 1998;178:53‐60. - PubMed
-
- Nair H, Brooks WA, Katz M, et al. Global burden of respiratory infections due to seasonal influenza in young children: a systematic review and meta‐analysis. Lancet. 2011;378:1917‐1930. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
