

Comparative study of lung and extrapulmonary poorly differentiated neuroendocrine carcinomas: A SEER database analysis of 162,983 cases
- PMID: 29211313
- PMCID: PMC5801102
- DOI: 10.1002/cncr.31124
Comparative study of lung and extrapulmonary poorly differentiated neuroendocrine carcinomas: A SEER database analysis of 162,983 cases
Abstract
Background: Extrapulmonary neuroendocrine carcinomas (NECs) are poorly studied and are managed similar to lung NECs, which may not account for differences between the 2 groups of tumors as well as the heterogeneity within extrapulmonary NEC.
Methods: Data from the Surveillance, Epidemiology, and End Results program between 1973 and 2012 were used to estimate the relative percentages of lung NECs and subgroups of extrapulmonary NECs, epidemiological patterns at these sites, and the median and 5-year overall survival rates.
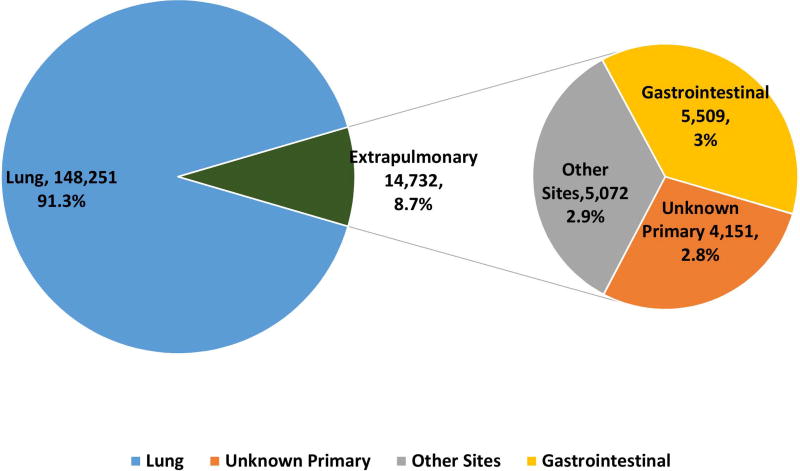
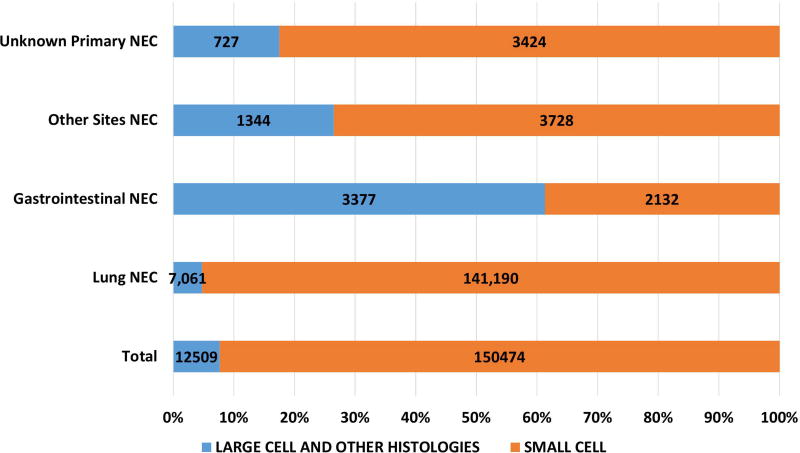
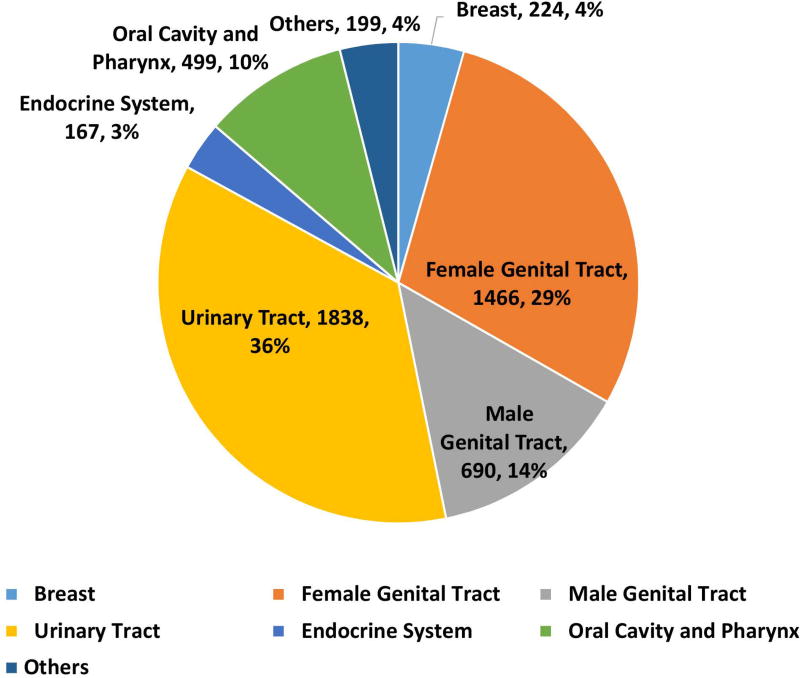
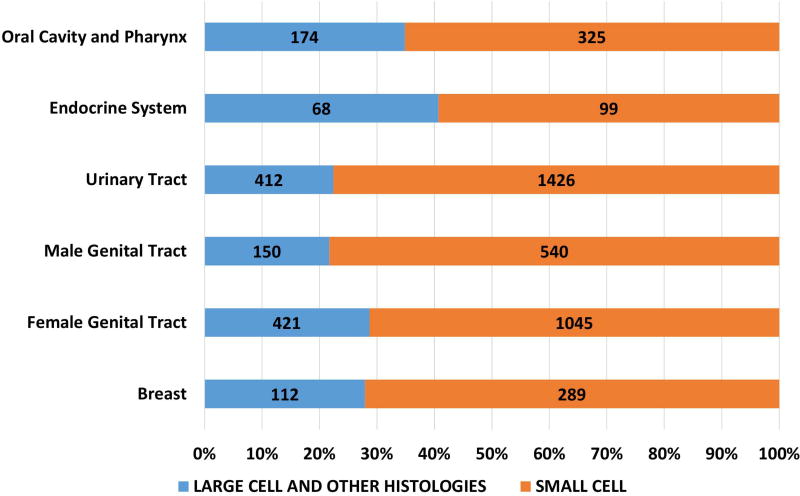
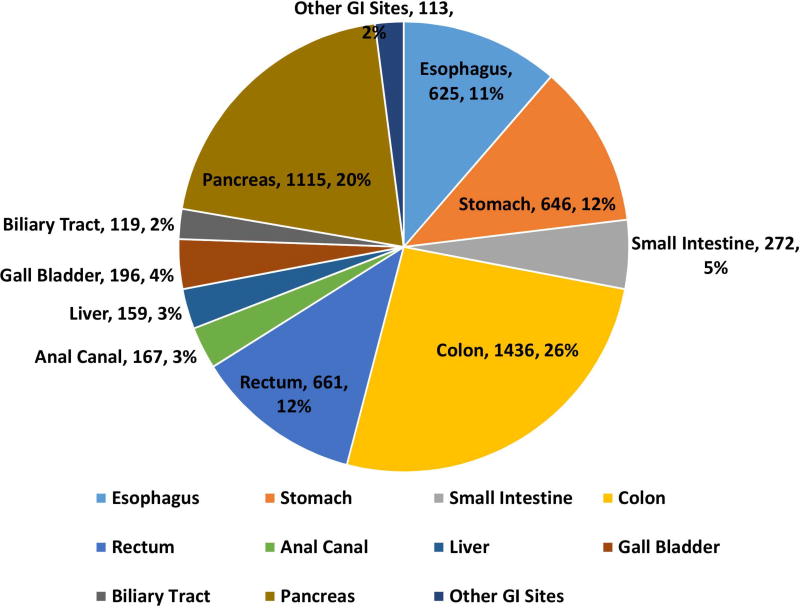
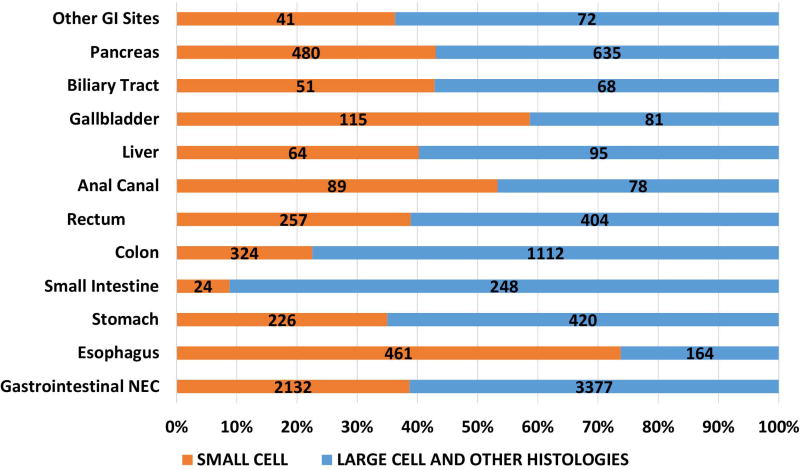
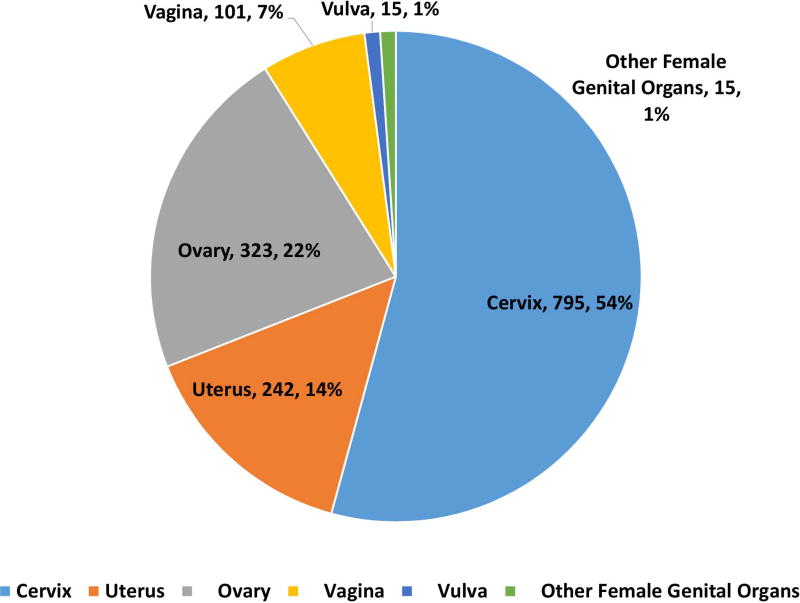
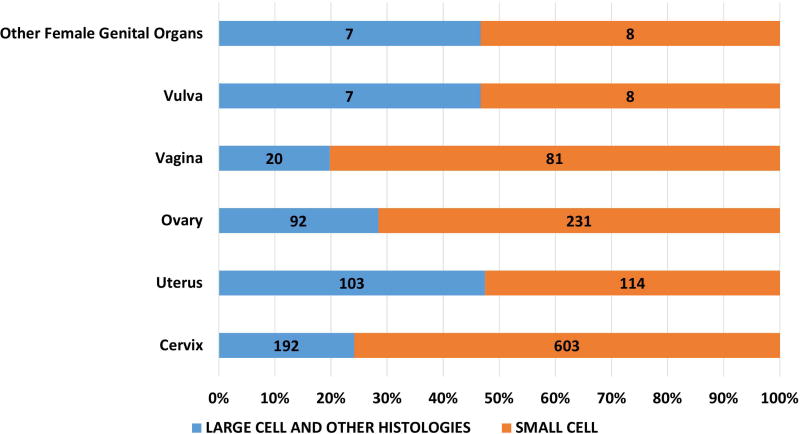
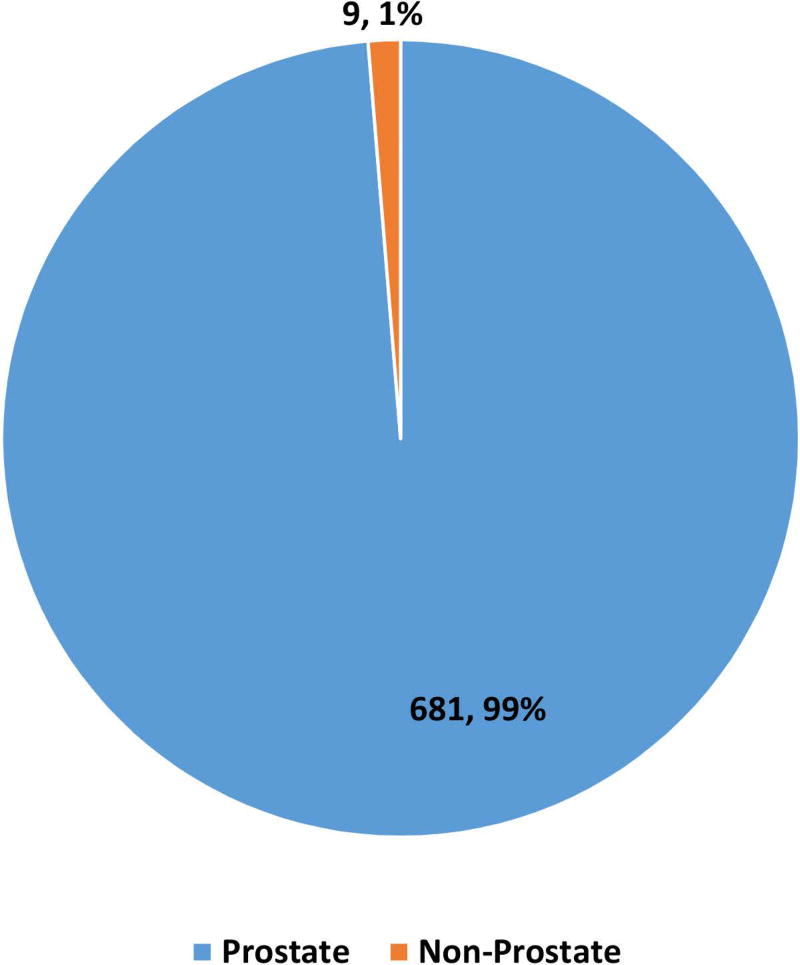
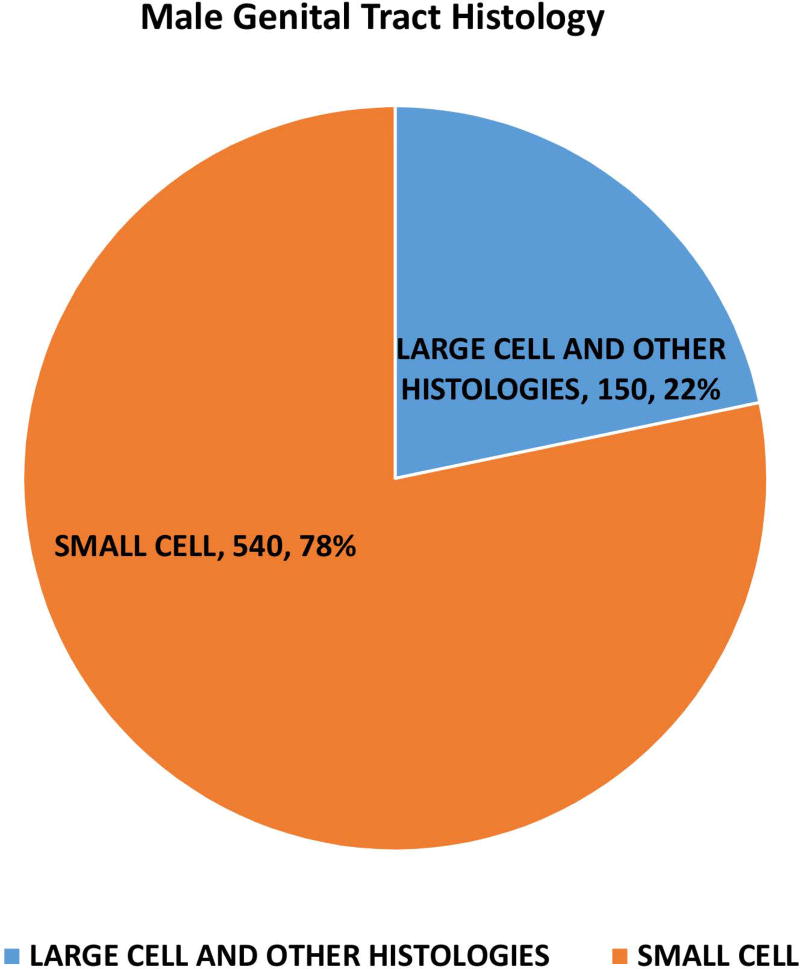
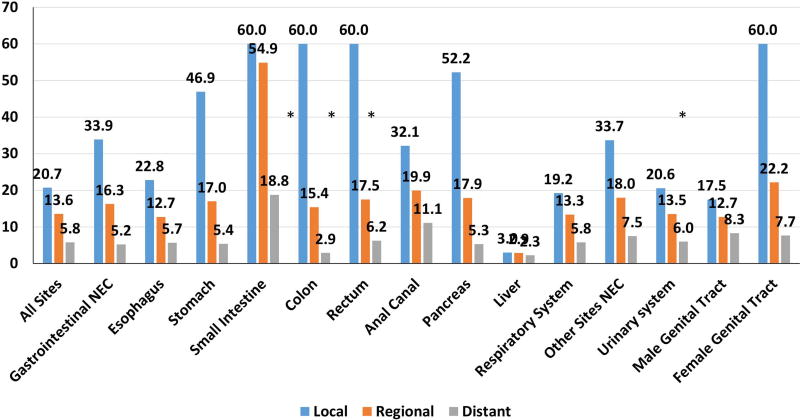
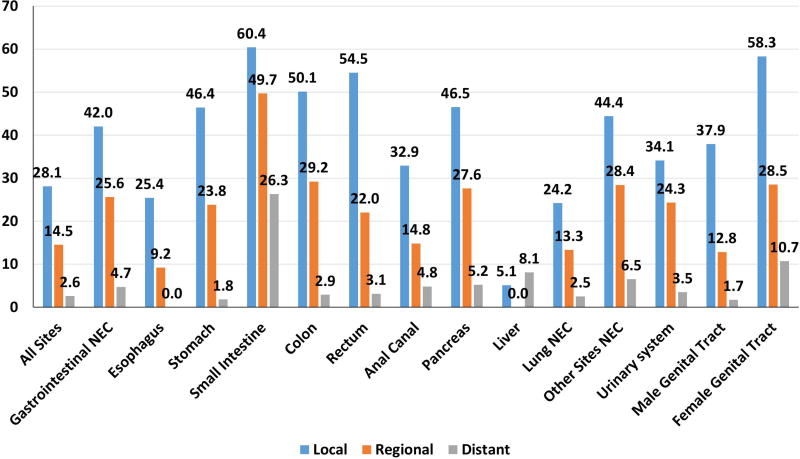
Results: Of 162,983 NEC cases, 14,732 were extrapulmonary; of these, 5509 were gastrointestinal (37.44%), 4151 were of unknown primary (28.2%), and 5072 were of other sites (34.4%). Lung NEC had the highest percentage of small cell morphology (95.2%) and gastrointestinal NEC had the least (38.7%), with the rest being other morphologies. Significant differences were noted with regard to median age (range, 48-74 years), percentage of cases of distant stage disease (24%-77%), and incidence according to sex and race. The median survival of patients with lung NEC was 7.6 months, that for patients with gastrointestinal NEC was 7.5 months (range, 25.1 months for NEC at the small intestine to 5.7 months for NEC at the pancreas), and that for patients with unknown NEC was 2.5 months. The 5-year survival rate for patients with local stage disease ranged from 58% to 60% for NECs of the female genital tract and small intestine to 25% for esophageal NECs. The primary tumor site remained statistically significant for survival even after adjusting for known prognostic variables (P<.0001).
Conclusions: To the authors' knowledge, the current study is the largest study of NECs performed to date and also the first with comprehensive epidemiological data. Significant differences in incidence patterns and large variations in survival depending on anatomical site and morphological subtype were noted. A curative approach is possible for patients with nonmetastatic NECs. Cancer 2018;124:807-15. © 2017 American Cancer Society.
Keywords: Epidemiology; Surveillance; and End Results (SEER); large cell; neuroendocrine carcinoma (NEC); poorly differentiated; small cell.
© 2017 American Cancer Society.
Conflict of interest statement
The authors have declared no conflicts of interest
Figures
References
-
- Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010;39(6):707–712. - PubMed
-
- Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol. 2015;10(9):1243–1260. - PubMed
-
- Soto DE, Eisbruch A. Limited-stage extrapulmonary small cell carcinoma: outcomes after modern chemotherapy and radiotherapy. Cancer J. 2007;13(4):243–246. - PubMed
-
- Ochsenreither S, Marnitz-Schultze S, Schneider A, et al. Extrapulmonary small cell carcinoma (EPSCC): 10 years' multi-disciplinary experience at Charite. Anticancer Res. 2009;29(8):3411–3415. - PubMed
-
- Kim JH, Lee SH, Park J, et al. Extrapulmonary small-cell carcinoma: a single-institution experience. Jpn J Clin Oncol. 2004;34(5):250–254. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
