

Update from a 12-Year Nationwide Fungemia Surveillance: Increasing Intrinsic and Acquired Resistance Causes Concern
- PMID: 29212705
- PMCID: PMC5869841
- DOI: 10.1128/JCM.01564-17
Update from a 12-Year Nationwide Fungemia Surveillance: Increasing Intrinsic and Acquired Resistance Causes Concern
Abstract
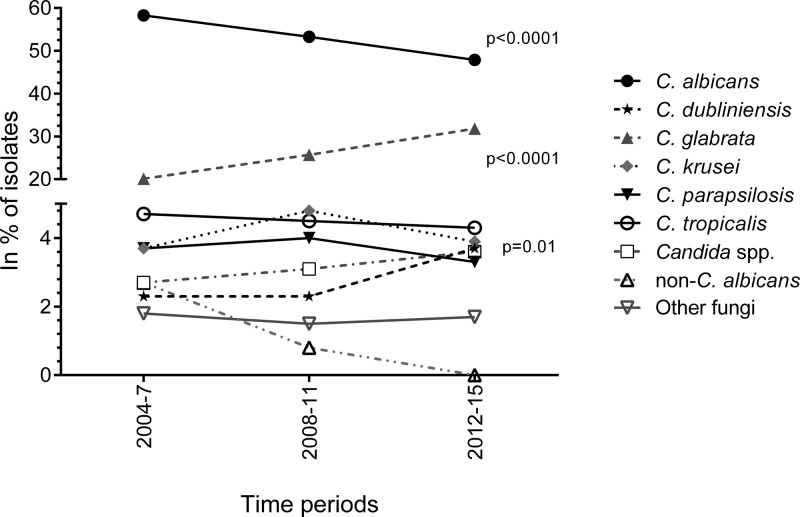
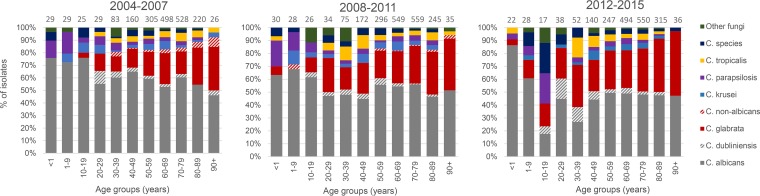
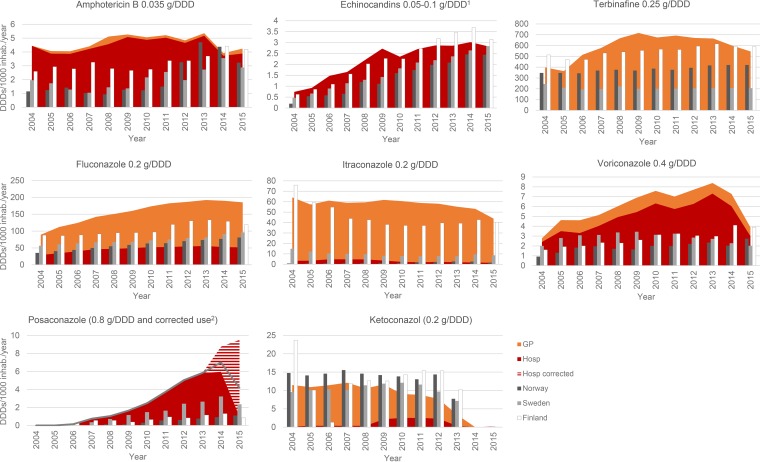
New data from the years 2012 to 2015 from the Danish National Fungemia Surveillance are reported, and epidemiological trends are investigated in a 12-year perspective (2004 to 2015). During 2012 to 2015, 1,900 of 1,939 (98%) fungal bloodstream isolates were included. The average incidence was 8.4/100,000 inhabitants, and this appears to represent a stabilizing trend after the increase to 10.1/100,000 in 2011. The incidence was higher in males than females (10.0 versus 6.8) and in patients above 50 years, and those changes were mainly driven by an increasing incidence among 80-to-89-year-old males (65.3/100,000 in 2014 to 2015). The proportion of Candida albicans isolates decreased from 2004 to 2015 (64.4% to 42.4%) in parallel with a doubling of the proportion of Candida glabrata isolates (16.5% to 34.6%, P < 0.0001). C. glabrata was more common among females (34.0% versus 30.4% in males). Following an increase in 2004 to 2011, the annual drug use stabilized during the last 2 to 3 years of that time period but remained higher than in other Nordic countries. This was particularly true for the fluconazole and itraconazole use in the primary health care sector, which exceeded the combined national levels of use of these compounds in each of the other Nordic countries. Fluconazole susceptibility decreased (68.5%, 65.2%, and 60.6% in 2004 to 2007, 2008 to 2011, and 2012 to 2015, respectively, P < 0.0001), and echinocandin resistance emerged in Candida (0%, 0.6%, and 1.7%, respectively, P < 0.001). Amphotericin B susceptibility remained high (98.7%). Among 16 (2.7%) echinocandin-resistant C. glabrata isolates (2012 to 2015), 13 harbored FKS mutations and 5 (31%) were multidrug resistant. The epidemiological changes and the increased incidence of intrinsic and acquired resistance emphasize the importance of continued surveillance and of strengthened focus on antifungal stewardship.
Keywords: Candida glabrata; antifungal consumption; azole resistance; candidemia; echinocandin resistance; epidemiology; fungemia; multidrug resistance; population-based; surveillance.
Copyright © 2018 American Society for Microbiology.
Figures

Comment in
-
Fungemia Surveillance in Denmark Demonstrates Emergence of Non-albicans Candida Species and Higher Antifungal Usage and Resistance Rates than in Other Nations.J Clin Microbiol. 2018 Mar 26;56(4):e01907-17. doi: 10.1128/JCM.01907-17. Print 2018 Apr. J Clin Microbiol. 2018. PMID: 29436419 Free PMC article.
References
-
- Lausch KR, Søgard M, Rosenvinge FS, Johansen HK, Boysen T, Røder BL, Mortensen KL, Nielsen L, Lemming LE, Olesen B, Leitz C, Kristensen L, Dzajic E, Østergård L, Schønheyder HC, Arendrup MC. 2017. Behind candidaemia: risk factors and outcome in a high-incidence nationwide setting, abstr OS0587 Abstr 27th ECCMID, 22 to 25 April 2017, Vienna, Austria.
-
- Lortholary O, Renaudat C, Sitbon K, Madec Y, Denoeud-Ndam L, Wolff M, Fontanet A, Bretagne S, Dromer F. 2014. Worrisome trends in incidence and mortality of candidemia in intensive care units (Paris area, 2002–2010). Intensive Care Med 40:1303–1312. doi: 10.1007/s00134-014-3408-3. - DOI - PMC - PubMed
-
- Puig-Asensio M, Padilla B, Garnacho-Montero J, Zaragoza O, Aguado JM, Zaragoza R, Montejo M, Muñoz P, Ruiz-Camps I, Cuenca-Estrella M, Almirante B. 2014. Epidemiology and predictive factors for early and late mortality in Candida bloodstream infections: a population-based surveillance in Spain. Clin Microbiol Infect 20:O245–O254. doi: 10.1111/1469-0691.12380. - DOI - PubMed
-
- Morrell M, Fraser VJ, Kollef MH. 2005. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother 49:3640–3645. doi: 10.1128/AAC.49.9.3640-3645.2005. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
