

Pharmacologic Prevention of Incident Atrial Fibrillation: Long-Term Results From the ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial)
- PMID: 29212812
- PMCID: PMC5728652
- DOI: 10.1161/CIRCEP.117.005463
Pharmacologic Prevention of Incident Atrial Fibrillation: Long-Term Results From the ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial)
Abstract
Background: Although atrial fibrillation (AF) guidelines indicate that pharmacological blockade of the renin-angiotensin system may be considered for primary AF prevention in hypertensive patients, previous studies have yielded conflicting results. We sought to determine whether randomization to lisinopril reduces incident AF or atrial flutter (AFL) compared with chlorthalidone in a large clinical trial cohort with extended post-trial surveillance.
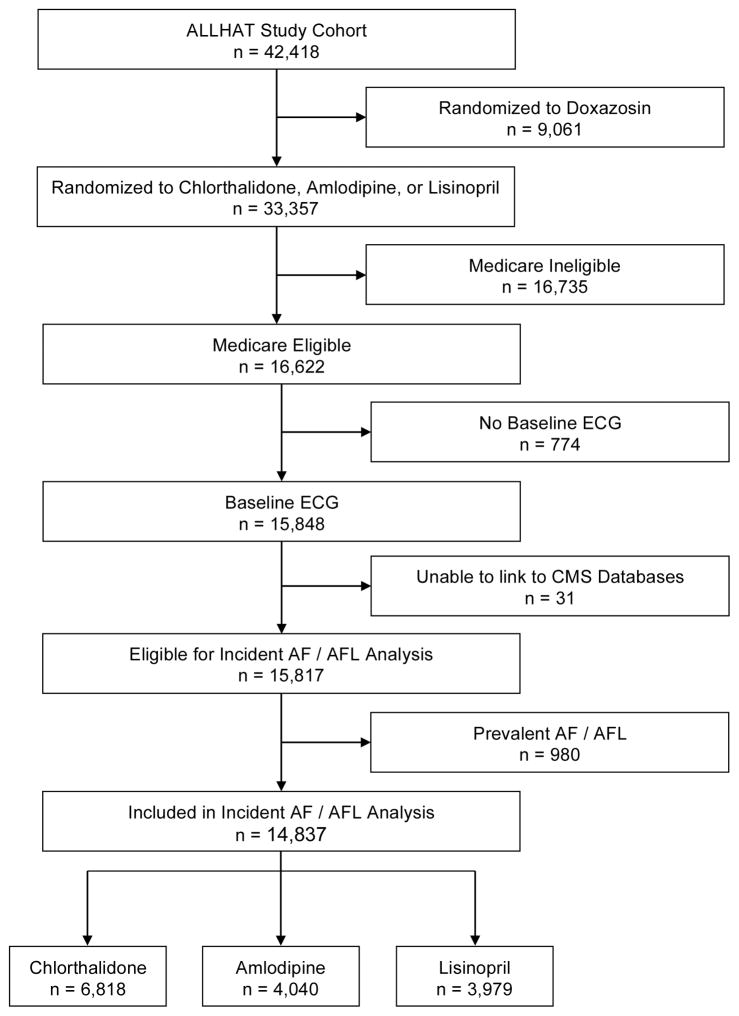
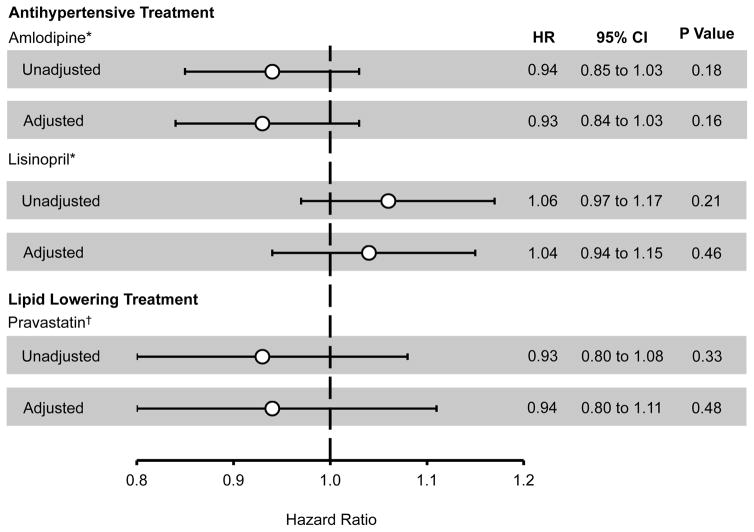
Methods and results: We performed a secondary analysis of the ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial), a randomized, double-blind, active-controlled clinical trial that enrolled hypertensive individuals ≥55 years of age with at least one other cardiovascular risk factor. Participants were randomly assigned to receive amlodipine, lisinopril, or chlorthalidone. Individuals with elevated fasting low-density lipoprotein cholesterol levels were also randomized to pravastatin versus usual care. The primary outcome was the development of either AF or AFL as diagnosed by serial study ECGs or by Medicare claims data. Among 14 837 participants without prevalent AF or AFL, 2514 developed AF/AFL during a mean 7.5±3.2 years of follow-up. Compared with chlorthalidone, randomization to either lisinopril (hazard ratio, 1.04; 95% confidence interval, 0.94-1.15; P=0.46) or amlodipine (hazard ratio, 0.93; 95% confidence interval, 0.84-1.03; P=0.16) was not associated with a significant reduction in incident AF/AFL.
Conclusions: Compared with chlorthalidone, treatment with lisinopril is not associated with a meaningful reduction in incident AF or AFL among older adults with a history of hypertension.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00000542.
Keywords: antihypertensive agents; atrial fibrillation; atrial flutter; primary prevention; renin-angiotensin system.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Atrial Fibrillation: Once Again Not So Easy to Prevent.Circ Arrhythm Electrophysiol. 2017 Dec;10(12):e005956. doi: 10.1161/CIRCEP.117.005956. Circ Arrhythm Electrophysiol. 2017. PMID: 29212813 No abstract available.
References
-
- Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol. 2009;104:1534–1539. - PubMed
-
- Lin HJ, Wolf PA, Kelly-Hayes M, Beiser AS, Kase CS, Benjamin EJ, D’Agostino RB. Stroke severity in atrial fibrillation. The Framingham Study. Stroke. 1996;27:1760–1764. - PubMed
-
- Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–952. - PubMed
-
- Wolowacz SE, Samuel M, Brennan VK, Jasso-Mosqueda J-G, Van Gelder IC. The cost of illness of atrial fibrillation: a systematic review of the recent literature. Europace. 2011;13:1375–1385. - PubMed
-
- Marcus GM. Predicting incident atrial fibrillation: an important step toward primary prevention. Arch Intern Med. 2010;170:1874–1875. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
