

Neuroimaging in normal pressure hydrocephalus
- PMID: 29213984
- PMCID: PMC5619317
- DOI: 10.1590/1980-57642015DN94000350
Neuroimaging in normal pressure hydrocephalus
Abstract
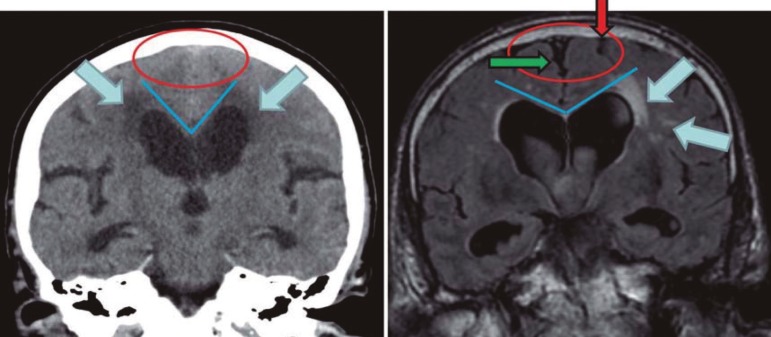
Normal pressure hydrocephalus (NPH) is a syndrome characterized by the triad of gait disturbance, mental deterioration and urinary incontinence, associated with ventriculomegaly and normal cerebrospinal fluid (CSF) pressure. The clinical presentation (triad) may be atypical or incomplete, or mimicked by other diseases, hence the need for supplementary tests, particularly to predict postsurgical outcome, such as CSF tap-tests and computed tomography (CT) or magnetic resonance imaging (MRI). The CSF tap-test, especially the 3 to 5 days continuous external lumbar drainage of at least 150 ml/day, is the only procedure that simulates the effect of definitive shunt surgery, with high sensitivity (50-100%) and high positive predictive value (80-100%). According to international guidelines, the following are CT or MRI signs decisive for NPH diagnosis and selection of shunt-responsive patients: ventricular enlargement disproportionate to cerebral atrophy (Evans index >0.3), and associated ballooning of frontal horns; periventricular hyperintensities; corpus callosum thinning and elevation, with callosal angle between 40º and 90º; widening of temporal horns not fully explained by hippocampal atrophy; and aqueductal or fourth ventricular flow void; enlarged Sylvian fissures and basal cistern, and narrowing of sulci and subarachnoid spaces over the high convexity and midline surface of the brain. On the other hand, other imaging methods such as radionuclide cisternography, SPECT, PET, and also DTI or resting-state functional MRI, although suitable for NPH diagnosis, do not yet provide improved accuracy for identifying shunt-responsive cases.
A hidrocefalia de pressão normal (HPN) é uma síndrome caracterizada por alteração da marcha, transtorno mental-cognitivo e incontinência urinária, associados a ventriculomegalia e pressão liquórica normal. A apresentação clínica (tríade) pode ser atípica ou incompleta, ou pode ser mimetizada por outras doenças, daí a necessidade de testes suplementares, principalmente para predição do resultado cirúrgico, tais como teste da punção lombar e tomografia computadorizada (TC) ou ressonância magnética (MR) de crânio. O teste da punção liquórica lombar, especialmente a drenagem externa contínua (≥150 ml/dia, por 3 a 5 dias), é o único método que simula o efeito da cirurgia, com alta sensibilidade (50-100%) e alto valor preditivo positivo (80-100%). Consensos internacionais consideram os seguintes achados da TC ou RM como decisivos para o diagnóstico de HPN e a seleção de pacientes bons respondedores à cirurgia: dilatação ventricular desproporcional em relação ao grau de atrofia cerebral (índice de Evans >0.3), associada a arredondamento dos cornos frontais; hipersinal difuso periventricular; adelgaçamento e elevação do corpo caloso, com ângulo do corpo caloso entre 40º e 90º; dilatação dos cornos temporais não explicada por atrofia hipocampal; sinal do fluxo vazio no aqueduto e quarto ventrículo; dilatação das fissuras Sylvianas e cisterna basal, e estreitamento ou apagamento dos sulcos e espaços subaracnoides nas superfícies cerebrais da convexidade alta e linha média. Por outro lado, a cisternografia isotópica, SPECT, PET, e mesmo técnicas mais modernas de RM funcional e tensor de difusão, embora compatíveis com o diagnóstico de HPN, não melhoram a acurácia na identificação de casos responsivos à cirurgia.
Keywords: cerebrospinal fluid tap test; magnetic resonance; neuroimaging; normal pressure hydrocephalus; shunt surgery.
Conflict of interest statement
Disclosure: The authors report no conflicts of interest.
Figures


Similar articles
-
Magnetic Resonance Imaging Diagnosis in Normal Pressure Hydrocephalus.World Neurosurg. 2024 Jan;181:171-177. doi: 10.1016/j.wneu.2023.10.110. Epub 2023 Oct 26. World Neurosurg. 2024. PMID: 37898265 Review.
-
The Utility of Neuroimaging Parameters in Discriminating Patients of Normal-Pressure Hydrocephalus with Positive Cerebrospinal Fluid Tap Test Response from Healthy Controls.Ann Indian Acad Neurol. 2020 Sep-Oct;23(5):625-631. doi: 10.4103/aian.AIAN_583_19. Epub 2020 Dec 8. Ann Indian Acad Neurol. 2020. PMID: 33623262 Free PMC article.
-
Normal pressure hydrocephalus: Diagnostic and predictive evaluationon.Dement Neuropsychol. 2009 Jan-Mar;3(1):8-15. doi: 10.1590/S1980-57642009DN30100003. Dement Neuropsychol. 2009. PMID: 29213603 Free PMC article. Review.
-
Absence of Disproportionately Enlarged Subarachnoid Space Hydrocephalus, a Sharp Callosal Angle, or Other Morphologic MRI Markers Should Not Be Used to Exclude Patients with Idiopathic Normal Pressure Hydrocephalus from Shunt Surgery.AJNR Am J Neuroradiol. 2019 Jan;40(1):74-79. doi: 10.3174/ajnr.A5910. Epub 2018 Dec 6. AJNR Am J Neuroradiol. 2019. PMID: 30523139 Free PMC article.
-
Preoperative prognostic value of MRI findings in 108 patients with idiopathic normal pressure hydrocephalus.AJNR Am J Neuroradiol. 2014 Dec;35(12):2311-8. doi: 10.3174/ajnr.A4046. Epub 2014 Jul 10. AJNR Am J Neuroradiol. 2014. PMID: 25012669 Free PMC article.
Cited by
-
Standardized regression-based clinical change score cutoffs for normal pressure hydrocephalus.BMC Neurol. 2020 Apr 16;20(1):140. doi: 10.1186/s12883-020-01719-y. BMC Neurol. 2020. PMID: 32299370 Free PMC article.
-
Common genetic variation influencing human white matter microstructure.Science. 2021 Jun 18;372(6548):eabf3736. doi: 10.1126/science.abf3736. Science. 2021. PMID: 34140357 Free PMC article.
-
Secondary parkinsonism associated with focal brain lesions.Front Neurol. 2024 Sep 4;15:1438885. doi: 10.3389/fneur.2024.1438885. eCollection 2024. Front Neurol. 2024. PMID: 39296961 Free PMC article. Review.
-
Standardized image evaluation in patients with idiopathic normal pressure hydrocephalus: consistency and reproducibility.Neuroradiology. 2019 Dec;61(12):1397-1406. doi: 10.1007/s00234-019-02273-2. Epub 2019 Aug 10. Neuroradiology. 2019. PMID: 31399851 Free PMC article.
-
Normal-pressure hydrocephalus: A critical review.Dement Neuropsychol. 2019 Apr-Jun;13(2):133-143. doi: 10.1590/1980-57642018dn13-020001. Dement Neuropsychol. 2019. PMID: 31285787 Free PMC article. Review.
References
-
- Krauss JK, Halve B. Normal pressure hydrocephalus: survey on contemporary diagnostic algorithms and therapeutic decision-making in clinical practice. Acta Neurochir (Wien) 2004;146:379–388. - PubMed
-
- Brean A, Eide PK. Prevalence of probable idiopathic normal pressure hydrocephalus (iNPH) in a Norwegian population. Acta Neurol Scand. 2008;118:48–53. - PubMed
-
- Tanaka N, Yamaguchi S, Ishikawa H, Ishii H, Meguro K. Prevalence of possible idiopathic normal pressure hydrocephalus in Japan: the Osaki-Tajiri project. Neuroepidemiology. 2009;32:171–175. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
