

Seven-Year Weight Trajectories and Health Outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) Study
- PMID: 29214306
- PMCID: PMC6584318
- DOI: 10.1001/jamasurg.2017.5025
Seven-Year Weight Trajectories and Health Outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) Study
Abstract
Importance: More information is needed about the durability of weight loss and health improvements after bariatric surgical procedures.
Objective: To examine long-term weight change and health status following Roux-en-Y gastric bypass (RYGB) and laparoscopic adjustable gastric banding (LAGB).
Design, setting, and participants: The Longitudinal Assessment of Bariatric Surgery (LABS) study is a multicenter observational cohort study at 10 US hospitals in 6 geographically diverse clinical centers. Adults undergoing bariatric surgical procedures as part of clinical care between 2006 and 2009 were recruited and followed up until January 31, 2015. Participants completed presurgery, 6-month, and annual research assessments for up to 7 years.
Main outcome and measures: Percentage of weight change from baseline, diabetes, dyslipidemia, and hypertension, determined by physical measures, laboratory testing, and medication use.
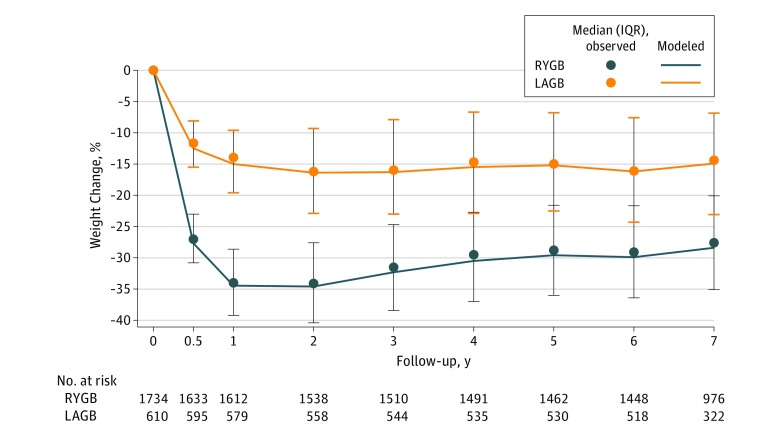
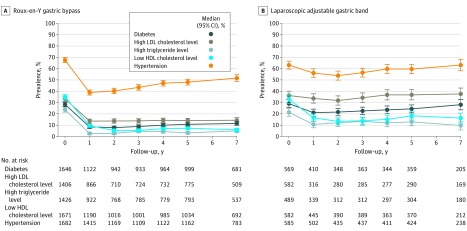
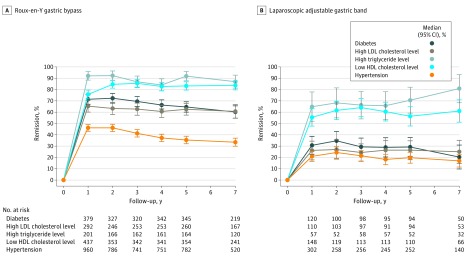
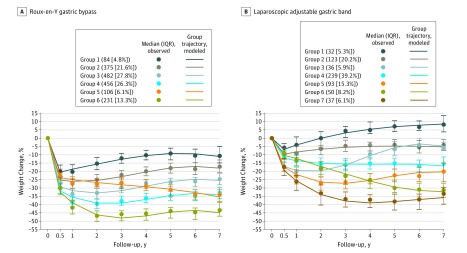
Results: Of 2348 participants, 1738 underwent RYGB (74%) and 610 underwent LAGB (26%). For RYBG, the median age was 45 years (range, 19-75 years), the median body mass index (calculated as weight in kilograms divided by height in meters squared) was 47 (range, 34-81), 1389 participants (80%) were women, and 257 participants (15%) were nonwhite. For LAGB, the median age was 48 years (range, 18-78), the body mass index was 44 (range, 33-87), 465 participants (76%) were women, and 63 participants (10%) were nonwhite. Follow-up weights were obtained in 1300 of 1569 (83%) eligible for a year-7 visit. Seven years following RYGB, mean weight loss was 38.2 kg (95% CI, 36.9-39.5), or 28.4% (95% CI, 27.6-29.2) of baseline weight; between years 3 and 7 mean weight regain was 3.9% (95% CI, 3.4-4.4) of baseline weight. Seven years after LAGB, mean weight loss was 18.8 kg (95% CI, 16.3-21.3) or 14.9% (95% CI, 13.1-16.7), with 1.4% (95% CI, 0.4-2.4) regain. Six distinct weight change trajectory patterns for RYGB and 7 for LAGB were identified. Most participants followed trajectories in which weight regain from 3 to 7 years was small relative to year-3 weight loss, but patterns were variable. Compared with baseline, dyslipidemia prevalence was lower 7 years following both procedures; diabetes and hypertension prevalence were lower following RYGB only. Among those with diabetes at baseline (488 of 1723 with RYGB [28%]; 175 of 604 with LAGB [29%]), the proportion in remission at 1, 3, 5, and 7 years were 71.2% (95% CI, 67.0-75.4), 69.4% (95% CI, 65.0-73.8), 64.6% (95% CI, 60.0-69.2), and 60.2% (95% CI, 54.7-65.6), respectively, for RYGB and 30.7% (95% CI, 22.8-38.7), 29.3% (95% CI, 21.6-37.1), 29.2% (95% CI, 21.0-37.4), and 20.3% (95% CI, 9.7-30.9) for LAGB. The incidence of diabetes at all follow-up assessments was less than 1.5% for RYGB. Bariatric reoperations occurred in 14 RYGB and 160 LAGB participants.
Conclusions and relevance: Following bariatric surgery, different weight loss patterns were observed, but most participants maintained much of their weight loss with variable fluctuations over the long term. There was some decline in diabetes remission over time, but the incidence of new cases is low following RYGB.
Trial registration: clinicaltrials.gov Identifier: NCT00465829.
Conflict of interest statement
Figures
Comment in
-
The Reality of Long-term Follow-up of Bariatric/Metabolic Surgery Patients-A Conundrum.JAMA Surg. 2018 May 1;153(5):435. doi: 10.1001/jamasurg.2017.5010. JAMA Surg. 2018. PMID: 29214300 No abstract available.
-
Considerations When Calculating Data Completeness.JAMA Surg. 2018 Aug 1;153(8):782. doi: 10.1001/jamasurg.2018.1159. JAMA Surg. 2018. PMID: 29799918 Free PMC article. No abstract available.
References
-
- Wolfe BM, Belle SH. Long-term risks and benefits of bariatric surgery: a research challenge. JAMA. 2014;312(17):1792-1793. - PubMed
-
- Sjöström L, Lindroos AK, Peltonen M, et al. ; Swedish Obese Subjects Study Scientific Group . Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351(26):2683-2693. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
